Home — Essay Samples — Nursing & Health — Anatomy & Physiology — Childbirth

Essays on Childbirth
Reviewing different childbirth techniques from several countries, research on the modern state of the childbirth, made-to-order essay as fast as you need it.
Each essay is customized to cater to your unique preferences
+ experts online
The Effects of Acupressure on Labor Pains During Childbirth
Medicalization of pregnancy and childbirth: the general goals and performance, defying nature: choosing the sex of an unborn baby is wrong , the factors of postpartum depression, let us write you an essay from scratch.
- 450+ experts on 30 subjects ready to help
- Custom essay delivered in as few as 3 hours
Child Birth
Evaluation on the decision on the life choice of having children or not, the role and significance of contraception in modern societies, differences and similarities in birth rituals and beliefs of the samoans and pygmies, get a personalized essay in under 3 hours.
Expert-written essays crafted with your exact needs in mind
Analysis of Margaret Sanger’s Speech on Birth Control
The intervention birth plan review, preimplantation and stages of fetus development, life beginning & fertalization, women’s age at first child’s birth, the importance and major developments in neonatology, the positive outcomes of childbirth at an older age, mary breckinridge and the history of nurse-midwifery, the efficacy of telephone-based lactation counseling: literature review, the effectiveness of birth control, the benefits of over the counter birth control, the population puzzle: understanding total fertility rate, the legal landscape of surrogacy: complexities and considerations, home births and societal perceptions, women's empowerment and choice in birth practices, reclaiming birth: the comprehensive exploration of home births, relevant topics.
- Human Physiology
- Cardiovascular System
- Digestive System
- Human Anatomy
- Homeostasis
- Pathophysiology
- Human Brain
By clicking “Check Writers’ Offers”, you agree to our terms of service and privacy policy . We’ll occasionally send you promo and account related email
No need to pay just yet!
We use cookies to personalyze your web-site experience. By continuing we’ll assume you board with our cookie policy .
- Instructions Followed To The Letter
- Deadlines Met At Every Stage
- Unique And Plagiarism Free
- Fact sheets
- Facts in pictures
- Publications
- Questions and answers
- Tools and toolkits
- Endometriosis
- Excessive heat
- Mental disorders
- Polycystic ovary syndrome
- All countries
- Eastern Mediterranean
- South-East Asia
- Western Pacific
- Data by country
- Country presence
- Country strengthening
- Country cooperation strategies
- News releases
- Feature stories
- Press conferences
- Commentaries
- Photo library
- Afghanistan
- Cholera
- Coronavirus disease (COVID-19)
- Greater Horn of Africa
- Israel and occupied Palestinian territory
- Disease Outbreak News
- Situation reports
- Weekly Epidemiological Record
- Surveillance
- Health emergency appeal
- International Health Regulations
- Independent Oversight and Advisory Committee
- Classifications
- Data collections
- Global Health Estimates
- Mortality Database
- Sustainable Development Goals
- Health Inequality Monitor
- Global Progress
- World Health Statistics
- Partnerships
- Committees and advisory groups
- Collaborating centres
- Technical teams
- Organizational structure
- Initiatives
- General Programme of Work
- WHO Academy
- Investment in WHO
- WHO Foundation
- External audit
- Financial statements
- Internal audit and investigations
- Programme Budget
- Results reports
- Governing bodies
- World Health Assembly
- Executive Board
- Member States Portal
- Activities /
Making childbirth a positive experience
The clinical management of labour and childbirth is well understood, but not enough attention is given to making women feel safe, comfortable and positive about their experience.
As well as providing essential information on clinical requirements for preventing and managing maternal mortality and morbidity, WHO prioritises the psychological and emotional needs of women giving birth.
In some settings, women are receiving too many interventions too late; in other settings women receive too many interventions that they may not need, too soon. WHO addresses safe and appropriate use of caesarean sections, promoting an environment that involves women in decision making and averts mistreatment during childbirth in health facilities.
Maternal health mirrors the gap between the rich and the poor. WHO insists that a positive childbirth experience should meet a woman’s personal and sociocultural beliefs and expectations in every setting.
This includes giving birth to a healthy baby in a clinically and psychologically safe environment, assisted by a kind and technically competent health care provider.
Countries commit to recover lost progress in maternal, newborn & child survival
New series highlights the importance of a positive postnatal experience for all women and newborns
More than a third of women experience lasting health problems after childbirth, new research shows
Climate change is an urgent threat to pregnant women and children
Relevant publications

WHO labour care guide: user’s manual
The WHO Labour Care Guide is a tool that aims to support good-quality, evidence-based, respectful care during labour and childbirth, irrespective of the...

WHO recommendations: non-clinical interventions to reduce unnecessary caesarean sections
Caesarean section is a surgical procedure that can effectively prevent maternal and newborn mortality when used for medically indicated reasons. Caesarean section...

WHO recommendations: intrapartum care for a positive childbirth experience
This up-to-date, comprehensive and consolidated guideline on essential intrapartum care brings together new and existing WHO recommendations that, when...

Pregnancy, childbirth, postpartum and newborn care: A guide for essential practice (3rd edition)
Pregnancy, childbirth, postpartum and newborn care: a guide for essential practice (3rd edition) (PCPNC), has been updated to include recommendations...
Infographics

All women have a right to a positive childbirth experience

Labour progression at 1 cm/hr during the active first stage may be unrealistic for some

Every birth is unique

WHO Labour Care Guide to support intrapartum care for a positive birth experience

Intrapartum care for a positive childbirth experience
Related work.
Strengthening quality midwifery for all mothers and newborns

Related WHO Teams
Related health topics
Maternal health
Newborn health
IELTS Essay: Childbirth
by Dave | Real Past Tests | 8 Comments

This is an IELTS writing task 2 sample answer essay on the topic of childbirth and advantages and disadvantages of having children when older from the real IELTS exam.
Please consider supporting me on Patreon.com/howtodoielts to receive my exclusive IELTS Ebooks – you can even sign up for private live lessons with me!
People nowadays tend to have children at older ages.
Do the advantages of this outweigh the disadvantages?
There are growing numbers of men and women choosing to have children later in life these days. In my opinion, the financial advantages of this trend far outweigh any perceived downsides.
The most significant tradeoffs of this relate to opportunity and maturity. Many individuals decide early on in their career to wait until their mid to late 30s to have children. The natural risk here is that if the relationship ends before that point or they then have trouble conceiving, they may end up childless. This possibility is lower today due to advances in fertility science but still exists. Furthermore, having children is a maturing experience. If an individual waits until late in life to raise a child, then they delay the experience gained and may later regret their decision. Most parents would openly admit that parenthood is a life-altering milestone and defining moment of adulthood.
Nonetheless, the disadvantages detailed above pale in comparison to the economic merits of delaying childbirth. Firstly, most young parents are not in an ideal situation in their career. Many working parents earn low salaries and work long hours. Once they have a child that means the majority of their day is occupied and they may feel trapped and overburdened. It is then difficult to switch careers or move to a new location as well as afford all the expenses incumbent on parents. This often results in parents becoming resentful and projecting their animosity towards their children or significant other. In contrast, parents who are firmly established in their careers, earn decent salaries, and have savings set aside have both the time and energy to devote to raising their children well without having to stress about making ends meet.
In conclusion, despite marginal risks concerning the opportunity and experience, it is an overall positive for financial reasons that many prospective parents are putting off childbirth. Therefore, this trend should be welcomed and encouraged.
1. There are growing numbers of men and women choosing to have children later in life these days. 2. In my opinion, the financial advantages of this trend far outweigh any perceived downsides.
- Paraphrase the overall essay topic.
- Write a clear opinion. Read more about introductions here .
1. The most significant tradeoffs of this relate to opportunity and maturity. 2. Many individuals decide early on in their career to wait until their mid to late 30s to have children. 3. The natural risk here is that if the relationship ends before that point or they then have trouble conceiving, they may end up childless. 4. This possibility is lower today due to advances in fertility science but still exists. 5. Furthermore, having children is a maturing experience. 6. If an individual waits until late in life to raise a child, then they delay the experience gained and may later regret their decision. 7. Most parents would openly admit that parenthood is a life-altering milestone and defining moment of adulthood.
- Write a topic sentence with a clear main idea at the end.
- Explain your main idea.
- Develop it with specific examples.
- Keep developing it fully.
- Stay focused on the same main idea.
- Use hypotheticals.
- Conclude with a strong statement.
1. Nonetheless, the disadvantages detailed above pale in comparison to the economic merits of delaying childbirth. 2. Firstly, most young parents are not in an ideal situation in their career. Many working parents earn low salaries and work long hours. 3. Once they have a child that means the majority of their day is occupied and they may feel trapped and overburdened. 4. It is then difficult to switch careers or move to a new location as well as afford all the expenses incumbent on parents. 5. This often results in parents becoming resentful and projecting their animosity towards their children or significant other. 6. In contrast, parents who are firmly established in their careers, earn decent salaries, and have savings set aside have both the time and energy to devote to raising their children well without having to stress about making ends meet.
- Write a new topic sentence with a new main idea at the end.
- Explain your new main idea.
- Include specific details and examples.
- Continue developing it…
- as fully as possible!
- Vary long and short sentences.
1. In conclusion, despite marginal risks concerning the opportunity and experience, it is an overall positive for financial reasons that many prospective parents are putting off childbirth. 2. Therefore, this trend should be welcomed and encouraged.
- Summarise your main ideas.
- Include a final thought. Read more about conclusions here .
What do the words in bold below mean? Make some notes on paper to aid memory and then check below.
There are growing numbers of men and women choosing to have children later in life these days. In my opinion, the financial advantages of this trend far outweigh any perceived downsides .
The most significant tradeoffs of this relate to opportunity and maturity . Many individuals decide early on in their career to wait until their mid to late 30s to have children. The natural risk here is that if the relationship ends before that point or they then have trouble conceiving , they may end up childless . This possibility is lower today due to advances in fertility science but still exists. Furthermore , having children is a maturing experience . If an individual waits until late in life to raise a child , then they delay the experience gained and may later regret their decision. Most parents would openly admit that parenthood is a life-altering milestone and defining moment of adulthood .
Nonetheless , the disadvantages detailed above pale in comparison to the economic merits of delaying childbirth . Firstly, most young parents are not in an ideal situation in their career. Many working parents earn low salaries and work long hours . Once they have a child that means the majority of their day is occupied and they may feel trapped and overburdened . It is then difficult to switch careers or move to a new location as well as afford all the expenses incumbent on parents. This often results in parents becoming resentful and projecting their animosity towards their children or significant other . In contrast, parents who are firmly established in their careers, earn decent salaries , and have savings set aside have both the time and energy to devote to raising their children well without having to stress about making ends meet .
In conclusion, despite marginal risks concerning the opportunity and experience, it is an overall positive for financial reasons that many prospective parents are putting off childbirth . Therefore , this trend should be welcomed and encouraged .
For extra practice, write an antonym (opposite word) on a piece of paper to help you remember the new vocabulary:
growing numbers more and more people
later in life when they are older
financial advantages good for your money
trend pattern
far outweigh are much stronger than
perceived downsides apparent disadvantages
significant tradeoffs major downsides
opportunity chance
maturity experience
decide early on choose from the beginning
mid to late 30s 35 – 40 years old
natural risk obvious threat
before that point prior to that
trouble conceiving difficulty having kids
may end up childless might finally not have kids
possibility chance
advances developments
fertility science medicine related to having kids
furthermore moreover
maturing experience makes you more like an adult
raise a child help a kid grow up
delay wait until later
regret wish it had been different
openly admit honestly say
parenthood being a parent
life-altering milestone significant moment in life
defining moment significant time
adulthood being an adult
nonetheless regardless
detailed above described over
pale in comparison to not as important as
economic merits helps you make money
delaying childbirth waiting until later to have kids
ideal situation best context
earn low salaries make more money at work
work long hours spend a lot of time at work
majority most of
occupied time taken up
trapped stuck
overburdened too much work
switch careers change jobs
location place
afford pay for
expenses incumbent on money you have to pay
results in causes
resentful annoyed
projecting putting on to someone else
animosity resentment
significant other partner, husband, wife
firmly established solidly in place
earn decent salaries make a lot of money
savings set aside money saved
devote to put time into
without having to not needing to
making ends meet earning enough money to survive
despite marginal risks regardless of small dangers
concerning related to
overall positive good on the whole
prospective parents possible parents later
putting off childbirth delaying having children
therefore thus
welcomed should be applauded
encouraged motivated
Pronunciation
Practice saying the vocabulary below and use this tip about Google voice search :
ˈgrəʊɪŋ ˈnʌmbəz ˈleɪtər ɪn laɪf faɪˈnænʃəl ədˈvɑːntɪʤɪz trɛnd fɑːr aʊtˈweɪ pəˈsiːvd ˈdaʊnˌsaɪdz sɪgˈnɪfɪkənt treɪd ɒfs ˌɒpəˈtjuːnɪti məˈtjʊərɪti dɪˈsaɪd ˈɜːli ɒn mɪd tuː leɪt 30 ɛs ˈnæʧrəl rɪsk bɪˈfɔː ðæt pɔɪnt ˈtrʌbl kənˈsiːvɪŋ meɪ ɛnd ʌp ˈʧaɪldlɪs ˌpɒsəˈbɪlɪti ədˈvɑːnsɪz fə(ː)ˈtɪlɪti ˈsaɪəns ˈfɜːðəˈmɔː məˈtjʊərɪŋ ɪksˈpɪərɪəns reɪz ə ʧaɪld dɪˈleɪ rɪˈgrɛt ˈəʊpnli ədˈmɪt ˈpeərənthʊd laɪf-ˈɔːltərɪŋ ˈmaɪlstəʊn dɪˈfaɪnɪŋ ˈməʊmənt əˈdʌlthʊd ˌnʌnðəˈlɛs ˈdiːteɪld əˈbʌv peɪl ɪn kəmˈpærɪsn tuː ˌiːkəˈnɒmɪk ˈmɛrɪts dɪˈleɪɪŋ ˈʧaɪldbɜːθ aɪˈdɪəl ˌsɪtjʊˈeɪʃən ɜːn ləʊ ˈsæləriz wɜːk lɒŋ ˈaʊəz məˈʤɒrɪti ˈɒkjʊpaɪd træpt ˌəʊvəˈbɜːdnd swɪʧ kəˈrɪəz ləʊˈkeɪʃən əˈfɔːd ɪksˈpɛnsɪz ɪnˈkʌmbənt ɒn rɪˈzʌlts ɪn rɪˈzɛntfʊl prəˈʤɛktɪŋ ˌænɪˈmɒsɪti sɪgˈnɪfɪkənt ˈʌðə ˈfɜːmli ɪsˈtæblɪʃt ɜːn ˈdiːsnt ˈsæləriz ˈseɪvɪŋz sɛt əˈsaɪd dɪˈvəʊt tuː wɪˈðaʊt ˈhævɪŋ tuː ˈmeɪkɪŋ ɛndz miːt dɪsˈpaɪt ˈmɑːʤɪnəl rɪsks kənˈsɜːnɪŋ ˈəʊvərɔːl ˈpɒzətɪv prəsˈpɛktɪv ˈpeərənts ˈpʊtɪŋ ɒf ˈʧaɪldbɜːθ ˈðeəfɔː ˈwɛlkəmd ɪnˈkʌrɪʤd
Vocabulary Practice
I recommend getting a pencil and piece of paper because that aids memory. Then write down the missing vocabulary from my sample answer in your notebook:
Listening Practice
Learn more about this topic in the video below and practice with these activities :
Reading Practice
Read more about this topic and use these ideas to practice :
https://www.theatlantic.com/health/archive/2017/05/how-people-decide-whether-to-have-children/527520/
Speaking Practice
Practice with the following speaking questions from the real IELTS speaking exam :
Talkative Children
- Do think being talkative is a good quality for children?
- Is it good for children to talk a lot in every situation?
- Why do children talk so much?
- What makes children talk less as the get older sometimes?
- What can teachers do to encourage children to talk more?
Writing Practice
Practice with the same basic topic below and then check with my sample answer:
Parents should take courses in parenting in order to improve the lives of their children.
To what extent do you agree?
IELTS Essay: Parenting
Recommended For You
Latest IELTS Writing Task 1 2024 (Graphs, Charts, Maps, Processes)
by Dave | Sample Answers | 147 Comments
These are the most recent/latest IELTS Writing Task 1 Task topics and questions starting in 2019, 2020, 2021, 2022, 2023, and continuing into 2024. ...
Recent IELTS Writing Topics and Questions 2024
by Dave | Sample Answers | 342 Comments
Read here all the newest IELTS questions and topics from 2024 and previous years with sample answers/essays. Be sure to check out my ...

Find my Newest IELTS Post Here – Updated Daily!
by Dave | IELTS FAQ | 18 Comments

IELTS Essay: Celebrities and Charity
by Dave | IELTS Writing Task 2 Real Past Tests Sample Answers | 0 Comment
This is an IELTS writing task 2 sample answer essay that is only available on my Patreon based on a real question from the exam. ...

IELTS Essay: Childhood Obesity
by Dave | EBooks | 0 Comment

IELTS Essay: Competition in University
by Dave | Real Past Tests | 0 Comment
This is an IELTS writing task 2 sample answer essay on the topic of the benefits and disadvantages of competition in university from the real IELTS ...
Submit a Comment Cancel reply
You must be logged in to post a comment.

Dear Dave, thank you very much for your essays!
May I ask you for advice? In this “advantages/disadvantages” type of essays, is it okay to mention only one advantage and one disadvantage? I find it really hard to mention 2 advantages and 2 disadvantages and fully develop my response with explanations and examples, it’s too lengthy!
Let’s say that in this essay, in the first body paragraph, I only say that there are ”physical challenges” and then I talk about how hard it is to give birth at a later stage. Is saying ”physical challenges” equivalent to saying that there are more than one disadvantage even though technically I only talk about one (which is the risk to human body when giving birth later in life)? Similarly, with the advantages I only talk about ”financial stability” which I can rephrase and call ”economic merits” as you did in your essay.
Is that okay for a body paragraph structure or do we have to mention at least 2 points in each paragraph because the task said ”disadvantageS outweigh advantageS”? [It’s impossible in 40 minutes!]
Thank you very much in advance!

I would not take that risk.
I think it is unfair and agree with you that students will have a tough time developing 4 total ideas. If I would change the test I would, but I can’t and I know there are examiners who will mark you down to a 4/5 for TA because you just develop one advantage or disadvantage (others won’t).
To be on the safe side, have two of each of course the examiner will understand the development will be less.
The way I get around it that you noticed is I have one general main idea and then develop a couple of adv/disadv within that – such as relating to finances. That’s the approach I recommend for students who can do it.
Thank you very much, Dave, for your wise advice! I’ll stay on the safe side and try to practice more with this type of questions. Thank you for your kindness!
You’re welcome!
Dear Dave, could you please look at this sample? Do body paragraphs look a bit choppy and abrupt (because they do to me)? Advantages/Disadvantages essays are incredibly difficult for me as the balance between ”too general” and ”too detailed” isn’t clear at times. Did I develop my ideas fully? I typed this essay in 30 minutes (in paper version I will need more time, that’s why I saved 10 extra minutes).
It is increasingly common these days to have children later in life. While there are some disadvantages associated with physical challenges, I believe that advantages far outweigh drawbacks.
The majority of trade-offs relate to physical issues concerned with raising a child. First, giving birth to the child is a hazardous act, when undertaken at a later stage in life. The mortality rate among aging parents, for instance, was much lower in the past, when children were born to families as early as possible. This, however, can still be prevented with the development of modern medicine. Second, raising a child may be considered physically demanding since kids require attention, and one has to be fit and strong to meet the child’s needs. Activities, such as playing games, escorting the kid to a kindergarten, or attending a doctor’s office demand a certain level of physical effort.
Nevertheless, there are still advantages associated with parents’ financial stability and maturity. First, older parents are more firmly established in their careers and, therefore, find it easier to cover all the necessary expenses. These might range from quite mediocre, such as clothing and nutrition, to more elaborate ones, including tuition fees and accommodation. Second, mature parents are more experienced and possess greater wisdom about life so that they can assist the children in the process of growing up. Their children might find it useful to get advice regarding life-altering choices, such as choosing a partner, or deciding on their career.
In conclusion, although there are certain setbacks associated with later childbirth, they can still be overcome by the use of science and medicine. Therefore, advantages detailed above can justifiably outweigh the drawbacks.
I think you are striking a really good balance in your writing and should keep doing what you are doing.
Most students who write 2 ideas in a paragraph, don’t develop one of them but you develop them fully and the detailing is very specific.
Keep it up – don’t change the way you are writing!
Dear Dave, thank you sooooo much! I can’t tell you how much I appreciate that, you really saved my life!
No problem – best of luck on your exam!
Exclusive Ebooks, PDFs and more from me!
Sign up for patreon.
Don't miss out!
"The highest quality materials anywhere on the internet! Dave improved my writing and vocabulary so much. Really affordable options you don't want to miss out on!"
Minh, Vietnam
Hi, I’m Dave! Welcome to my IELTS exclusive resources! Before you commit I want to explain very clearly why there’s no one better to help you learn about IELTS and improve your English at the same time... Read more
Patreon Exclusive Ebooks Available Now!
Essays on Childbirth
Faq about childbirth.
Hektoen International
A Journal of Medical Humanities

Changes in childbirth in the United States: 1750–1950
Laura Kaplan New York, New York, United States
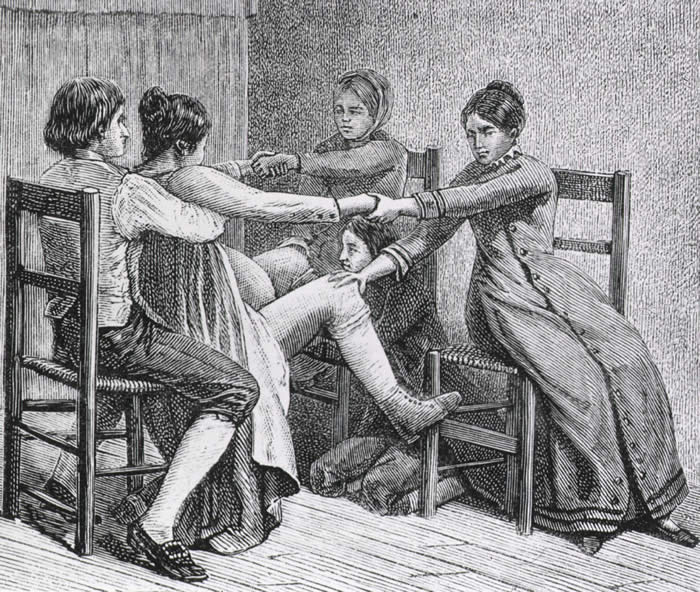
Gustave Joseph Witkowski Wood print From Histoire des accouchements chez tous les peuples
For most of American history, pregnancy, labor and delivery, and post-partum have been dangerous periods for mother and child. However, starting slowly in the late 18 th century and accelerating into the late 19 th century, labor and delivery radically changed. Initially new medical interventions, such as forceps and anesthesia, caused as many issues as they seemed to resolve as they emerged in burgeoning medical school obstetric programs. But the introduction of standard physician training accompanied by an emphasis on infection control eventually led to substantially decreased morbidity and mortality in the mid-20 th century. From a home-based event managed by female midwives and other birth attendants without formal training to a hospital-based, standardized encounter managed by formally trained male and female physicians and other healthcare practitioners, this complete paradigm shift resulted from women’s determination to have a safe and painless delivery, a new scientific foundation, innovations in medicine, and changes in the social landscape. (Fig 1)
Until the 20 th century, the majority of US births occurred in the home, attended by female midwives and numerous female family and friends. As no formal training programs, curricula, licensing processes, or other official standards for birth attendants existed until the 18 th century, women learned to help and support their loved ones through their own and others’ birth experiences. Historically, midwives—a diverse group of female community members who were usually married with children of their own—learned their skills by delivering their neighbors’ children or through loose apprenticeships with more established midwives. Only after the 1860s did some midwives begin attending midwifery schools. Midwives tended to intervene as minimally as possible and worked to assist labor along its natural course. Yet childbirth and the postpartum period long remained times of high morbidity and mortality. 1,2
As American women in the 18 th and 19 th centuries had on average seven live births during their lifetimes—and potentially a number of undocumented early terminations—women’s diaries and letters reveal the considerable time women spent preparing for the pain and the realistic possibility of dying in childbirth. One 19 th century woman wrote to her family late in her pregnancy: “If I live and regain my health, I will surely write to [all the people to whom she owed letters].” 1 In 1885, another wrote about her third birth, “Between oceans of pain, there stretched continents of fear; fear of death and a dread of suffering beyond bearing.” 1 In addition, women who survived childbirth and the postpartum period frequently suffered from lifelong morbidities, such as vesicovaginal and rectovaginal fistulas from unrepaired lacerations. The resulting lifelong incontinence and vaginal, cervical, and perineal prolapses of these fistulas caused painful sexual intercourse and difficulties with future pregnancies. A physician noted in 1897, “the wide-spread mutilation . . . is so common, indeed, that we scarcely find a normal perineum after childbirth.” 1 Despite numerous uncertainties inherent in childbearing into the 20 th century, American women persevered to control the process through the selection of childbirth attendants, preferring to deliver in a comfortable, safe setting (sometimes traveling back to their childhood home). 1
American women first invited male physicians to assist in birthing rooms in the 1760s. 1 Previously, physicians, who were exclusively male, were rarely called except in extreme emergencies, and men were excluded from attendance unless women were unavailable. In 1762, Dr. William Shippen, Jr. of Philadelphia, after training in midwifery in London and Edinburgh, became the first American male physician to establish a normal obstetrics practice in the US. Shippen also pioneered formal midwifery education through a lecture series initially taught to both male physicians and female midwives, but later limited to male physicians. Other physicians subsequently offered courses in other large American cities, and medical schools progressively incorporated obstetric education into their curricula.
As numbers of physicians formally trained in midwifery increased through the 19 th century, the wealthy, urban elite—who perceived male physicians as superior in education and training—were progressively more inclined to pay the higher physician fees, presuming that the physician’s modern interventions would result in safer childbirth. Such women chose their physician attendants similarly to how they had chosen their midwife attendants. For instance, at the turn of the century, records showed that midwife birth attendants in both rural and urban Wisconsin primarily attended the labor of local women of similar ethnic backgrounds. For deliveries, city midwives in Milwaukee and Madison rarely traveled beyond wards contiguous to their own, and rural midwives rarely worked outside their township. 2 Similarly, physicians tended to be from their immediate communities and of similar ethnic backgrounds. Even with the rise of railroad lines and automobiles in the 20 th century, physicians’ practice areas did not significantly expand. 2
New medical interventions that physicians employed—such as forceps, anesthesia, and laceration repair—increased the popular perception of the increased safety being provided in childbirth. 1,3 In the early 19 th century, the physicians’ primary interventions were forceps for difficult deliveries, bloodletting to relieve pain and accelerate labor, ergot to stimulate contractions, and drugs (particularly opium) for pain relief. 1 The forceps were invented in the 1590s by Peter Chamberlen the Elder, a French Huguenot “male midwife” whose family had fled to England. Peter was one of the most famous male midwives in England, serving as the queen’s surgeon and delivering the children of multiple kings. He and his family kept the forceps as a family secret for over a century, reportedly performing deliveries under a sheet or blanket to guard their creation.
In the early 18 th century, other practitioners developed their own versions of forceps, Dr. William Smellie of Scotland being the most well-known. Smellie taught midwifery and systemically described the proper use of forceps, publishing Treatise on the Theory and Practice of Midwifery in 1752. 1,3 With the introduction of forceps, physicians were able to extract fetuses that had previously been undeliverable, which mothers viewed as miraculous. However, as no standards existed for when forceps should be employed, 19 th century physicians were generally improperly trained in their use. As a result, individual practices differed substantially, and interventions frequently caused new problems. Some physicians used forceps routinely in every delivery even though their misapplication resulted in increased perineal lacerations, uterine trauma, and fetal defects. There was great debate among American physicians about the proper use and abuse of forceps throughout the 19 th century. 1
The introduction of anesthesia in the mid-19 th century was a key milestone in the history of obstetrics. Based on reading of thousands of diaries and letters from parturient American women from the 18 th and 19 th centuries, Judith Walzer Leavitt concluded that “next to the fear of death, pain was probably the single part of birth most hated by birthing women.” 1 After the first public demonstration of ether in 1846 by dentist William Morton at Massachusetts General Hospital in Boston, 4 Fanny Appleton Longfellow was the first woman to use it during childbirth in 1847, writing, “I feel proud to be the pioneer for less suffering for poor, weak womankind. This is certainly the greatest blessing of this age.” 1 Subsequently, wealthy women pressed physicians to use ether and chloroform to decrease their suffering. As with forceps, proper use of anesthesia was not standardized, and practice and debate varied tremendously about all aspects of its use, including when and whether to initiate it and appropriate dosing. Consequently, improper anesthetic use caused numerous complications, particularly prolonged labor due to decreased ability of the uterus to contract, newborn breathing difficulty, and hemorrhage. 1
Due to the limitations of ether and chloroform, women and their physicians searched for a superior anesthetic. 5 In the early 20 th century, Austrian and German physicians—followed by American physicians a few years later—began experimenting with a combination of scopolamine and morphine in childbirth. Alone, scopolamine acts an as amnesic, erasing all later memory of childbirth. Given with an opiate, it also has an anesthetic effect. Scopolamine-morphine, named “twilight sleep,” permitted the patient to be semiconscious with intact contractions during labor, allowing the physician to coach the woman through childbirth without her remembering the experience afterwards. In 1914, McClure’s magazine published “Painless Childbirth,” in which two laywomen raved about German Drs. Karl Gauss and Bernhardt Kronig’s twilight sleep protocol, but lamented the American physician’s inadequate training in the method.

Immediately, a vocal contingent of American women embraced and advocated for twilight sleep for their deliveries, and numerous articles and books were published on the subject. 5 From 1914–1915, the National Twilight Sleep Association—organized by wealthy upper- and middle-class women and led by prominent leaders such as Dr. Bertha Van Hoosen in Chicago and Mrs. Francis X. Carmody—advocated relentlessly for physicians and women to adopt twilight sleep, which allowed painless childbirth. In the words of Mrs. Carmody: “the twilight sleep is wonderful but, if you women want it you will have to fight for it, for the mass of doctors are opposed to it.” 5 As with other innovations, twilight sleep suffered from widespread controversy over in the medical community and enormous discrepancy in practice. Despite the drug’s amnesic effects, women under scopolamine still experienced intense labor pains, screaming and thrashing so much during labor that they were placed in “crib beds” to avoid accidents. 1

By the summer of 1915, twilight sleep sharply declined in popularity. Inappropriate use of the drug by physicians had frequently led to adverse events, including maternal delirium and asphyxiation of newborns. Notably, in August 1915, Mrs. Carmody died in childbirth while under scopolamine’s influence. Her physicians and husband maintained that her death did not result from scopolamine use; however, her neighbor Mrs. Alice J. Olsen initiated a campaign against twilight sleep in response to the event. As the drug’s popularity decreased, doctors limited scopolamine use to the first stage of labor, when it was still considered safe. 5
Though the twilight sleep movement was brief, it had long-lasting repercussions. The drug’s promise of a painless childbirth propelled women and their physicians to increasingly seek drugs and other means to ensure that childbirth would be as painless as possible. 1 This pursuit, in the context of the twilight sleep movement, brought many women—who otherwise would have chosen home deliveries—to the hospital to avoid numerous problems with home scopolamine administration.
As infection was one of the leading causes of postpartum death, infection control also attracted women to physician-attended labor in hospitals. 1 However, while American Dr. Oliver Wendell Holmes and Austrian Dr. Ignnaz Semmelweis recommended careful handwashing to prevent doctor-to-patient transmission of infection in the 1840s, it was Koch, Pasteur, and others’ revolutionary work on bacteria in the late 1860s that propelled the infection control movement in labor and delivery. By the 1880s, increasing numbers of physicians adopted infection control methods, though debates on the matter persisted for decades.
Early methods of antisepsis included vaginal chloral douches (injections of antiseptics into the vagina before and after delivery) and strict scrubbing of the genital area and physician’s hands (with numerous specific recipes and protocols). By the turn of the century, rubber gloves, a rubber “Kelly pad” (a rubber sheet placed under the patient for discharges), and shaving of the genital area were standard recommendations for practicing physicians. Initially, physicians tried to incorporate antisepsis as much as possible in home birthing rooms. However, in the first decades of the 20 th century, they began to encourage patients to come to hospitals for truly sterile births, as it was difficult to guarantee the cleanliness of the patient’s home and adherence of other birth attendants to their practices. 1
Other non-medical developments led to changes in women’s childbirth practices in the US, including the “mystification of medical knowledge” and the breakdown in women’s social networks for childbirth. With advances in obstetrics, women believed the promise of “science” could alleviate dangers and fears surrounding childbirth. Early 20 th century women’s journals and American women advised each other to select a trustworthy physician and follow his guidance, as he knew best. In addition, with increased mobility and urbanization in the 19 th and 20 th centuries, women no longer had the same expanded social support for pregnancy. The idea of a hospital where nurses and physicians took care of all of their needs was very appealing. 1
Hospital deliveries through the 1940s were entirely different from home deliveries, however. At home, the parturient exerted control over procedures and anesthesia administered by birthing attendants; in the hospital, women had no input into the drugs and procedures they received. Through the 1940s, hospital births frequently left women disillusioned and terrified, often contributing to psychiatric distress for extended periods after delivery. One woman wrote: “Months later I would scream out loud and wake up remembering that lonely labor room and just feeling no one cared what happened to me, no one kind reassuring word was spoken by nurse or doctor. I was treated as if I was an inanimate object.” 1
Interestingly, despite their promise, the numerous advances in obstetric medicine in the 19 th and first decades of the 20 th centuries did not immediately translate to improved safety during labor and the postpartum period. 1,2 Though hospital births were believed to be safer, there was no decrease in maternal mortality between hospital and home births until the 1940s. Despite strides in obstetric knowledge, practical training in medical school remained limited in the first decades of the 20 th century. Faculty lectures, student recitations, and practice with a manikin largely comprised the obstetric curriculum at most medical schools. While some schools had courses devoted to pelvic exams and delivery with and without obstetric instruments using a manikin, until 1900, the majority of medical students observed at most one to two deliveries in either the lecture hall or the patient’s home—and many never witnessed one. Famous obstetrician Dr. Joseph DeLee, who graduated from Northwestern, later recalled that he felt lucky to have observed two deliveries as a medical student.

The publications of the 1910 Flexner Report and Dr. J. Whitridge Williams of Johns Hopkins’s 1914 survey of American medical schools’ obstetrics departments both showcased medical schools’ failures in obstetric education. As a result, medical schools labored to increase the number of births witnessed by medical students. 1 For decades, this was an uphill battle. Consequently, new physicians continued to be poorly trained to handle deliveries, and practicing physicians still lacked standards of practice to ensure the safety of delivery interventions. 2 Lacking such standards, physicians during this period routinely over-utilized forceps, drugs to accelerate delivery, episiotomies, and other interventions—despite ongoing debate in the medical literature—in order to distinguish themselves from low-interventionalist midwives. Through the 1920s, mortality rates for midwife- and physician-assisted births remained similar, with physician assisted delivery possibly faring worse.
In the 1930s and 40s, American physicians—largely wealthy, native-born, white males—increasingly differentiated themselves from traditional midwives—chiefly working-class immigrants and African Americans—through standardized medical school curricula, formal credentials for practice, and professional societies with the authority for self-regulation. 1 In addition obstetric specialists also endeavored to establish obstetrics as its own hospital-based specialty, arguing that poorly trained general practitioners, who were “responsible for many obstetrical disasters” needed to cease obstetric work. In addition to establishing obstetrics’ role in the hospital, obstetric specialists redefined the medical philosophy of birth. Contrary to previous depictions of birth as a natural, though painful and dangerous, process, the new obstetricians, such as Dr. Joseph DeLee, deemed birth a “pathologic process” that required close medical supervision. Obstetric specialists formed professional associations, such as the American Congress of Obstetricians and Gynecologists (ACOG) in 1930. By 1936, ACOG was certifying specialists, with the authority to determine who could establish a hospital-based practice.
From the turn of the century on, women increasingly opted to deliver with physicians over midwives—initially with familiar community doctors and then with hospital-based physicians. In 1900, midwives still delivered half of all US births, but by 1930, this number dropped to less than 15% of US births, primarily in the South. 2 Similarly, in 1900, less than 10% of American births occurred in a hospital. By 1940, 26.7% of non-white and 55% of white American births took place in a hospital, increasing to 56% (non-white) and 88% (white) by 1950. 1 It was at the turn of the century, when births became more prevalent in the hospital, that physician-assisted birth no longer became the purview of the wealthy; very poor and/or single women who lacked other alternatives also utilized physicians as birth attendants. 1
During this period, physicians and hospitals learned to standardize obstetric practices to reduce mortality, such as appropriate use of drugs, proper indications and contraindications for obstetric procedures, and improved methods of antisepsis. Later developments of antibiotics, blood transfusions for hemorrhages, and prenatal care for high risk patients significantly contributed to the decline in maternal mortality. As maternal mortality rates fell in the 1940s and 1950s, women sought to regain some control, decision-making power, and humanity in the birth process that they had for millennia prior to the move to the hospital. In this environment, the natural childbirth movement and other philosophies of childbirth as a natural, normal process in which women possess control developed beginning in the 1950s–60s. 1
Birth in America changed dramatically from the colonial period to the 20 th century. The development of obstetrical “science” and numerous innovations including forceps, anesthesia, and antisepsis transformed childbirth into a standardized process that women no longer feared. Originally occurring at home in a familiar bed supported by female midwives, family, and friends, childbirth moved to a sterile hospital environment accompanied by male and female health professionals and select loved ones. By the middle of the 20 th century, these changes coincided with significant reductions in morbidity and mortality as a result of childbirth. By actively seeking safer and less painful childbirth and slowly allowing physicians and their developing technology to attend to them, parturient women changed the natural history and their personal experiences of childbirth.
- Judith Walzer Leavitt, Brought to Bed: Childbearing in America 1750–1950 (New York: Oxford University Press, 1986).
- Charlotte G. Borst, Catching Babies: The Professionalization of Childbirth (1870–1920) (Cambridge: Harvard University Press, 1995).
- J. Drife, “The Start of Life: A History of Obstetrics,” Postgraduate Medical Journal 78 (2002): 311–315, http://pmj.bmj.com/content/78/919/311.full.
- James F. Crenshaw and Elizabeth A. M. Frost, “The Discovery of Ether Anesthesia: Jumping on the 19th-century Bandwagon,” Archives of Family Medicine 2 (May 1993): 481–484.
- Amy Hairston, “The Debate Over Twilight Sleep: Women Influencing Their Medicine,” Journal of Women’s Health 5, no. 5 (1996), http://www.liebertonline.com/doi/pdf/10.1089/jwh.1996.5.489.
LAURA KAPLAN , MD, studied the history of science, medicine, and technology as an undergraduate at Johns Hopkins University and wrote this paper as a fourth-year medical student in Dr. Mindy Schwartz’s History of Medicine course at the University of Chicago. She is now a Family Medicine resident at Beth Israel Medical Center in New York.
Highlighted in Frontispiece Fall 2012 – Volume 4, Issue 4
Leave a Reply Cancel reply
Your email address will not be published. Required fields are marked *
This site uses Akismet to reduce spam. Learn how your comment data is processed .
- Open access
- Published: 03 November 2018
Childbirth experiences and their derived meaning: a qualitative study among postnatal mothers in Mbale regional referral hospital, Uganda
- Josephine Namujju ORCID: orcid.org/0000-0003-3408-9560 1 ,
- Richard Muhindo 1 ,
- Lilian T. Mselle 2 ,
- Peter Waiswa 3 , 4 ,
- Joyce Nankumbi 1 &
- Patience Muwanguzi 1
Reproductive Health volume 15 , Article number: 183 ( 2018 ) Cite this article
19k Accesses
32 Citations
11 Altmetric
Metrics details
Evidence shows that negative childbirth experiences may lead to undesirable effects including failure to breastfeed, reduced love for the baby, emotional upsets, post-traumatic disorders and depression among mothers. Understanding childbirth experiences and their meaning could be important in planning individualized care for mothers. The purpose of this study was to explore childbirth experiences and their meaning among postnatal mothers.
A phenomenological qualitative study was conducted at Mbale Regional Referral Hospital among 25 postnatal mothers within two months after birth using semi-structured interviews and focus group discussions and data was thematically analyzed.
The severity, duration and patterns of labour pains were a major concern by almost all women. Women had divergent feelings of yes and no need of biomedical pain relief administration during childbirth. Mothers were socially orientated to regard labour pains as a normal phenomenon regardless of their nature. The health providers’ attitudes, care and support gave positive and negative birth experiences. The Physical and psychosocial support provided comfort, consolation and encouragement to the mothers while inappropriate care, poor communication and compromised privacy contributed to the mothers’ negative childbirth experiences. The type of birth affected the interpretations of the birth experiences. Women who gave birth vaginally, thought they were strong and brave, determined and self-confident; and were respected by members of their communities. On the contrary, the women who gave birth by operation were culturally considered bewitched, weak and failures.
Childbirth experiences were unique; elicited unique feelings, responses and challenges to individual mothers. The findings may be useful in designing interventions that focus on individualized care to meet individual needs and expectations of mothers during childbirth.
Peer Review reports
Plain ENGLISH summary
Childbirth experiences are the women’s personal feelings and interpretations of birth processes. Birth experiences to some women have meant hard work, exciting lovely event and to others it is a stressful, exhausting and unpredictable experience. Negative experiences have been associated with poor support and care, fear, excessive pain, discomfort and undesirable outcomes. Participating in making decisions regarding childbirth care and being supported by healthcare providers gives a positive memory and increases the woman’s confidence and love for the baby and better adjustment to motherhood. Understanding the women’s childbirth experiences and their meaning is important in providing socially acceptable individualized care during and after birth. In Uganda, few studies on childbirth experiences of mothers and their meanings have been done. This study explored childbirth experiences and their meanings among women within two months after giving birth. Twelve women were interviewed one on one and thirteen women in two groups of seven and six in Mbale Regional Referral Hospital, in the Eastern part of Uganda. The women reported unique experiences of labour pains, they had social orientation on labour and gave different views on pain management during birth. Negative and positive attitudes and care by service providers were described and the social support from the significant others was noted as a source of comfort and encouragement. The personal women’s and society’s interpretations of birth experiences focused on the type of birth undergone. The vaginal birth meant braveness to some mothers and caesarean birth was associated with witchcraft and weakness of a woman. In conclusion, the individual mothers had unique childbirth experiences that required service provider’s understanding and personalized care.
Childbirth is a significant event in a woman’s life and a transition to motherhood. Childbirth experiences are the subjective psychological and physiological processes, influenced by the social and environmental factors [ 1 ]. Birth experiences elicit uncertainties of the next destination with feelings of inabilities [ 2 ]. Labour pain has been regarded as a “well kept – secret” whose true reality cannot be explained until you go through it causing fear and emotional upsets [ 3 ]. Childbirth is perceived as a paradox of moments of sadness and disappointment initially and joy crowns its end if a baby is alive [ 3 ]. The interpretations of birth experiences further include hard work, exciting intimate event and a stressful, exhausting and unpredictable phenomenon [ 4 ]. To some women, giving birth is life itself, a fulfillment of God’s plan and the law of procreation and a turning point between death and life for the woman and her baby [ 5 ].
Childbirth experiences could be both positive and negative. Negative experiences are characterized by fear, excessive pain, poor support and care, discomfort and undesirable outcomes [ 6 , 7 , 8 ]. The negative experiences of medical interventions like epidural analgesia, induction of labor and instrumental vaginal delivery have been found to be associated with post-traumatic stress, fear of childbirth, reduced child care and emotional upsets among women [ 7 , 9 ]. The positive memories of being in control over the situational happenings and the decisions on care coupled with the healthcare providers’ support are said to enhance self-confidence with feelings of accomplishment and better adjustment to motherhood [ 9 , 10 , 11 ]. The positive birth experiences are thus said to improve the bonding between the mother and the baby [ 12 , 13 , 14 ].
Understanding the women’s childbirth experiences and their meaning is crucial in the provision of individualized and culturally sensitive care during and after childbirth [ 15 , 16 , 17 ]. A number of studies have described women’s childbirth experiences and their meaning but these studies were done in the developed world. In Uganda, studies on childbirth experiences of mothers and the perceived meanings are scarce. This study therefore, describes the childbirth experiences and the perceived meanings among postnatal mothers seeking postnatal services at Mbale Regional Referral Hospital in Eastern Uganda to broaden the information base for appropriate intervention development and individualized care during childbirth.
Study design and setting
A phenomenological qualitative research design was used. Phenomenological qualitative research is an approach that describes life experiences and gives them meaning [ 18 ]. The design allows exploration of participants’ experiences, perspectives and feelings, in depth, through a holistic framework. Childbirth is a lived experience to women whose truth and reality is deeply embedded in the lives of those that have experienced it [ 19 , 20 ]. In this study, it was specifically used to explore experiences, feelings and perspectives of women who had given birth. The study was conducted at Mbale Regional Referral Hospital (MRRH) located in Mbale Municipality, Northeast of Kampala, Uganda. MRRH is a public hospital with 500 bed capacity. The hospital serves 13 districts (with about 4 million people in the region) and about 800 women give birth per month in this hospital. Specifically, the study was carried out at the Young Child Clinic (YCC), one of the clinics run by the Department of Obstetrics and Gynaecology in MRRH. The clinic had four certified health care providers including 3 midwives and 1 public health nurse. It offers immunization, health education, monitoring growth and development to children under 5 years; postnatal care services, HIV counseling and testing, and referral services for example HIV positive mothers and babies were being referred to the HIV clinic for care. On average, 35 mothers and babies were attended to at this clinic per day.
Participants and recruitment
Purposive sampling was used to recruit participants. Purposive sampling allows a researcher to get rich information to a particular research question [ 21 ]. The researcher oriented the staff of the YCC on the study and worked with the midwife in charge of the clinic to identify potential participants. The inclusion criteria were the postnatal mothers who gave birth within two months with live babies and those that were able to communicate in English, Luganda or Lumasaba. Luganda however, which all participants understood and spoke fluently was preferred in the two discussions. After receiving the services they had come for, all the potential participants were requested to meet with the researcher. She explained to them the study, its aim and how it was going to be conducted including their rights and the principles of confidentiality. Those who agreed to take part in the study gave written consent and a suitable place (with privacy) at hospital was arranged for an interview or discussion.
Data collection
To build the credibility and better understanding of the childbirth experiences two methods of data collection were used; the semi-structured interviews (SSI) and the focus group discussions (FGDs).
Semi-structured interviews
Twelve (12) semi-structured interviews with postnatal mothers were conducted in Luganda and English by the first author at YCC in a quiet room adjacent to the clinic. The saturation was reached with 12 interviews where the answers from mothers seemed to repeat information gained earlier with little new information [ 22 ] . A semi-structured interview guide with open ended questions and probes were used to explore and understand better the issues as they emerged [ 23 ] and elicited broader and deeper views from participants. All the interviews were audio recorded and lasted within 30 min.
Focus group discussions
Two FGDs with postnatal mothers were conducted. The discussion groups included 6 and 7 postnatal mothers. The first author moderated the discussions and notes and non-verbal clues were taken by the assistant, the clinic midwife who was not involved during the participants’ recruitment process. The FGD guide used centered on the mothers’ childbirth experiences and their meanings. The discussions were held in Luganda, the local language of instruction in schools, spoken and preferred by all participants and all the discussions were audio recorded with permission from participants. The discussions lasted between 60 and 80 min.
Data analysis
Thematic analysis guided the analysis of data. All the audio recorded interviews and discussions were transcribed verbatim and were translated from Luganda to English. The English translated transcripts were reviewed and edited to ensure correct interpretation of the mothers’ accounts. The analysis procedure included familiarization with the material through careful reading of sentence by sentence for many times, identification of the codes, searching for subcategories, formulation, revision and interpretation of themes. Phrases and sentences related to the mothers’ experiences of childbirth were coded in the margin of the transcript sheets. The coding was predominantly close to the text using mothers’ own descriptions. The codes with similar content were then brought together into sub-categories and themes. The authors discussed and reflected on the interpretations of the mothers’ descriptions of their childbirth experiences and agreed on the themes. Anonymous quotes were used to illustrate the facts.
Methodological considerations
Qualitative researchers suggest the use of credibility, transferability, dependability and conformability as methods to ensure trustworthiness in qualitative studies [ 24 , 25 ]. The researcher ensured credibility through use of multiple data collection methods (focus group discussions and in depth-interviews) which allowed triangulation of findings. Also the researcher established good rapport through having prolonged engagement in the field, used Luganda language (during FGDs) to build trust with participants. Bracketing was done through the researcher’s honest self-examination of the values, beliefs, interests and prior experiences. These were noted down and kept at the back of the mind right from proposal development through data collection, analysis and report writing to ensure that the findings were the views of the participants and not the researcher’s imaginations.Dependability and conformability were promoted through inquiry audit where by the researchers reviewed and examined the research process and the data analysis in order to ensure that the findings were consistent. Further, the thick description of the phenomenon under study, the purposive sampling used, the data collection methods that were employed and using participant’s own words during analysis and write up enhance the understanding of childbirth experiences and will allow for others to determine its transferability to other contexts [ 26 ] .
The 25 women who were interviewed about their childbirth experiences described themselves as housewives ( n = 7), teachers ( n = 6), business women (n = 6), students ( n = 2), a journalist, an administrator, a peasant and health information assistant ( n = 1). They were between 18 and 33 years of age, 88% ( n = 22) were married; 88% (n = 22)gave birth in the health facilities and 12% delivered at their homes or from the traditional birth attendant. Their parity ranged from one to five and the majority were Christians (Born again (32%), Protestants (24%), Catholics (12%), the rest were Moslems (32%).
From the 12 semi-structured interviews and 2 focus group discussions, five (5) themes emerged. These included the Childbirth experiences (Labour pains and management, Institutional care and support, Childbirth fears and Social support) and the Meaning attached to childbirth experiences (Individual and Cultural interpretations). The Women reported diverse trends in their birth experiences that provided the differences and the basis for emphasis. Numbers were used to identify participants during group discussions instead of names for privacy purposes and fictive names are used in the presentation of quotes.
Childbirth experiences
Labour pains and management.
The memory of labour pains remained in the minds of almost all women and formed the basis for their stories. The women’s birth pain experiences were viewed and expressed in terms of intensity, duration and patterns. The severe labour pains to some women were characterized by the temporary moments of confusion and loss of understanding as one mother expressed:
This is the 4 th born, other children never pained me like this one,…contractions were very strong and I reached a point when I did not understand well, they just lifted me up on to the bed. ….I just found myself delivered. After delivering, my senses came back (Zaifa, 27 years, a mother of 4)
Rose who experienced abnormal labour patterns also said:
Labour for my last born was hard, because the pains were much and later the contractions stopped. …..later the midwives put on a drip for contractions (Rose, 30 years, a mother of 4).
Some womenexperienced labour for a long duration and its effects were reported with dismay, frustration and loss of hope as one mother explained:
…the contractions pained me for 3 days… I went back, they examined me … I was still not ready. I walked and walked …. I went back at 6.00pm (second day, I was still not ready. I went back at 10.00 p.m, they told me I was not ready. I went back at midnight, the midwife told me, aaaah we are fed up with you, you go and walk so that the baby can move down, …the body was feeling like a metal, I said this time I am dead ( Eseza, 23years, a mother of one) .
The labour pain aspect of childbirth is one dimension that is given attention in various ways. In this study, the women were socially oriented to view labour pains as a normal phenomenon regardless of intensity, duration and varying patterns. This psychological care in preparation for birth provided consolation, hope and encouragement as narratives below indicate:
“ My attendants told me, contractions pain but you must be strong, and when time comes for the baby to come out, the baby itself will force you ” (Shifa, a 28 year old mother of 2).
“Getting much pain happens and is human and normal to a woman, but it is God who gives you the life and energy” (Rehema, a 33 year old mother of five) .
Labour pain management elicited mixed feelings from participants. Some women believed childbirth is natural and therefore should be left to take the natural course, while others felt it was necessary to reduce on the birth pains through medication if it was possible. According to the women’s descriptions, none of them received biomedical painkillers during birth and one mother explained:
Next time I deliver, I would not want to have too much labour pains like the ones I went through. If that medicine was there, I would feel like having such a drug to reduce the pain (Christine, 25 years, a first time mother).
Some women doubted as to whether medicine could have an effect on a natural process like labour pains as they had no prior knowledge to the intervention
“I think no need of medicine, because it is natural. I think even if they give you some medicine for pain, contractions would still come because the baby has to come out. I think the drugs cannot reduce those pains…every other woman goes through that” (Irene, 26 years, a primepara) .
Institutional care and support
The experiences of women regarding care and support received in the health facilities varied from positive by some mothers to negative and non-satisfying by others. Regarding institutional births, majority of women had given birth from the Regional Referral Hospital apart from one woman who had delivered from a private maternity centre. The women’s comments generally centred on the attitude of service providers, the interpersonal communication, the physical and psychological support and how the labour complications were managed. For those who felt good about their labour experiences described them in form of the good reception and attention given to them, the physical and psychological support through counseling; being listened to and having been given appropriate management to the complications as some mothers narrated:
The midwives were good…. even when they were attending to other people, when I would also call her (musawo) meaning a health care provider, also come and help me, She would not shout at me, would say let me come, I am hearing. I used to hear that they shout at people but for me they never shouted at me. ( Christine, a 25 year old mother of one).
Another one said:
The midwives welcomed me well, examined me … delivery time had not reached. I told them, basawo, I am sick, (HIV positive) they said you have done a good thing to tell us…, they said don’t fear. Some hide and do not tell us. ….when the time reaches you will push well and in case something wrong happens, we will help you. When time came, the midwife helped me to climb the bed. After delivery, I bled a lot … quickly they ran and gave me an injection and blood stopped. … weighed the baby, wrote treatment and gave the syrup for the baby ( Rehema, a 33year mother of 5 ).
As some mothers expressed their birth experiences with confidence and trust in service providers, to others it was a moment of reflection on the sadness, suffering and agony they went through. The women described experiences of non- caring attitude, limited technical care and support; quarreling and being rough to them. Rose,one of the mothers that was cared for by the morning and evening ward staff described her experience with the midwife of the 2nd shift:
…. I called her that I feel like something pushing me, she never bothered. She said, “Keep quiet, for you, you are making yourself tired for nothing, you are not going to deliver now”. I forced to deliver myself, what can I do? (Voice tone lowered) I said that if I relax I would lose my baby…. When the midwife reached, the baby was out and a lot of water (liquor) had poured on the baby. She (midwife) got annoyed, quarreled…. She cut the baby’s cord from that water yet I normally see midwives cut the cord from the mother’s abdomen. I felt too bad.
The practices reflected by some health care providers were unethical and violated the rights of the clients as one mother who was slapped during the time she pushed her baby narrated:
… the midwife told me to push. I tried to push and push, she was even slapping me telling me to push. The old woman (attendant) had given the midwife some money, now she was on my “bamper” (on my neck). “I have told you to push the baby with slaps” (Ruth, a 20 year old mother of 2)
Giving birth by caesarean was a hurdle. One mother who was taken to the theatre for the caesarean birth experienced delay to be operated as theatre was unready causing her stress and anxiety. This was heighted by being left exposed naked, a factor that compromised her privacy as she lamented:
….now you are under stress and you feel like… they have to do it (operation) immediately. “They take you in the theatre room, you again spend some good time there when they are still organizing. It was too bad, ….now even you feel stress is coming back again , you try to console yourself , you control…As you wait, you are naked, you are exposed there… (laughed while shaking her head)… you know how funny it is. ..you are nude. It was not good, privacy was not enough”. (Caroline, a 30 year old mother of 3 children).
Many women were giving birth for the first time and as such needed more information regarding labour and its proceedings. Women noted limited effective communication and sharing of information by the service providers. The non-involvement of a mother in decision-making regarding her care resulted in a number of unanswered questions as one woman explained:
….. the doctor told me, Irene, with you, you are just going for an operation. …I had to break down… because I was like what has gone wrong? ... why not me to deliver like other women? ….they are telling me I am going for an operation but they are not telling me the cause! Doctor Just told me, the baby was big. He then used some medical language that I did not understand. She did not convince me as to why I should have an operation… they were talking alone! (Irene, a first time mother).
Social support
The mothers according to their narratives appreciated the presence, proximity, the physical and psychological support from their birth companions that were basically family members (the mums, sisters, mothers-in law, aunties, husbands) and friends. Physically, the women were supported by giving them food and drinks like tea, they were supported to walk around before reaching second stage of labour and their backs were rubbed to provide relief during contractions by their birth companions.
Eseza a 23 year old mother of 3 recounted:
Attendants (birth companions ) helped me to get tea to drink, they kept around, and during that time when I could get the contractions, they could support me at the back, rub it, I could get some relief of about one minute.
Irene, a 26 year old primepara, who was supported through counselling by a relative before a caesarean birth recalled:
“At that time when I broke down,… my sister in law and mother in law were there for me. They tried to counsel and consoled me but still it wasn’t an easy moment”
The male partners were involved in intrapartum care of their spouses at different times and in various ways. Although their (male partners’) physical presence was registered at the hospital, their participation in real care was minimal. One mother whose husband was in hospital but at a distance from the maternity unit commented:
My husband was not near, had feared and moved away. I never wanted him to be near because when you are in labour the face changes, you may say that it is this one who brought the problems and get annoyed with him (laughed) (Shifa, a mother of 2).
Another mother whose husband fully participated in the processes of the birth of their baby by being present at the side of his partner and providing physical and psychological support during the pushing time gave her story:
When I came back to the labour ward they told me “the baby has reached you push”, I was not feeling any energy. ….my husband helped me, held me and he never feared. When the baby was coming out, he told me that “bambi” (meaning my friend) push more,the head is coming, add in more effort. … I felt good, I liked it so much because he gave me support,and he was there (Faith, a mother of one).
Childbirth fears
Childbirth is a moment of unpredictable “next” in terms of the outcome of the baby and mother both to those who give birth normally and by caesarean birth. In this study, these experiences were worsened by giving birth by a caesarean resulting into mothers’ fear, anxiety and loss of hope for survival as one woman recalled:
It is hard when you are going for a cesarean birth, you are always worried. …… you are not sure of what is going to happen there….. in such situation the mother is not sure of the baby’s survival and her own wellbeing; or she might come out with complications. Yah…it is like you are going for trouble when you are seeing (mother laughed) ( Catherine, a 30-year mother of 3, with 3 previous scars) .
The situation can be more terrifying to those who are giving birth for the first time. Irene, a first time mother had refused a caesarean birth for fear of losing her life in theatre until all hope of delivering normally was lost.
The doctor told me, “Irene, with you, you are just going for an operation at 10am”. ….I had to break down, I did not know … “if others can push normally, why not me?” At 10 a.m I refused the operation. I told them I don’t want, give me time ……I had feared the theatre because with me I knew whoever goes to theatre, does not come back. They just die like that. I imagined very many things
Multidimensional sources of fear were reported in this study. One mother who experienced excessive bleeding and a retained placenta regretted the decision she had made of delivering at home: “being with aunt alone I feared, I felt my life was going and regretted not having been in hospital”. The mistreatment of women by health care providers was sofrightening that one mother vowed never again to deliver in that hospital as she expressed it:
“... I forced to deliver myself”….in that difficulty situation I went through, I got scared, I feared the midwives of the main hospital (government). I feared too much, I said next time when I deliver, at least I go to private but not go back to main hospital. (Rose, a mother of 4 children) .
The negative stories (the past experiences by other mothers) about the institutional care were noted to be far reaching and a source of childbirth fears regarding the place of delivery. One mother who presumed and perceived hospital care negatively resorted to practices that undermine the quality of birth outcomes as she gave birth at the TBA’s home and gave her account:
“I refused going to hospital. I had no appetite of going there. What I hear threatened me. I hear in the hospital they don’t care about you, you care for yourself. ……..You are seeing this one is complaining, that one grumbling, another one is dying, I avoided such things. I said at least, for me let me die from here (TBA’s) and those other ones die there in hospital” (Amina, an 18-year-old primepara).
Meaning attached to childbirth experiences: The individual woman’s and societal interpretations
The individuals’ childbirth experience meaning.
The individual women interviewed had varying personal interpretations of their birth experiences. The sense made out of it was determined by what preoccupied the woman at that time of labour, the transpirations of the day and the outcomes. The supremacy of God in the event of childbirth was strongly expressed by many women but in union with self-belief and determination of an individual. The women were convinced that God had to be in control for a successful birth. One woman said; …. things to do with childbirth, it is God’s grace and others affirmed:
You must believe in yourself and believe in God. ….for me during birth, I said yes I will do it… I became firm and pushed the baby. Believing in yourself helps you to push the baby (Zaharah, 24 years, mother of one) .
“ It’s not an easy thing but when you are determined, God can be by your side, yah then you will get a child” (Irene, a 26-year-old first time mother).
As some women believed childbirth had a strong bearing on one’s personal effort put in during labour, to others birthing without complications was perceived and directly associated with “being strong and brave” as accounts below indicated:
.... people used to consider me as a weak person and thought I would not manage to give birth by myself… but I demonstrated that I am strong , (She stressed the point very happily, entire group went into laughter)…I pushed the baby without any problem (Amina, an 18 year old, primepara)
Anna, a 28-year-old first time mother also added:
“….. others when they start to push, they push and even die. I had to push and I saw the baby; then what I concluded is that i am brave because it is not easy there”
Societal and cultural interpretation of childbirth experiences
When women were asked to comment on how society perceived the different birth experiences they had gone through, the responses were cross cutting despite mothers being from different tribal and cultural backgrounds. The socio- cultural interpretations were mainly bent on the type of birth a woman went through. A mother was considered a strong woman if she gave birth well (vaginally) and the operated were regarded bewitched, failures or weak women.
Caroline, who had 3 consecutive operations said:
The Gisu’s themselves think that when you go for an operation, …. you are bewitched. …you are unable to have children, unable to be a real housewife; … not a good house woman to make a child for somebody.
Irene, a first- time mother who delivered by caesarean birth was insulted by the community members as she explained:
Culturally, to the illiterate, they assume whoever goes for an operation failed to push. You are a weak woman. So, they were insulting me “eeeh she had just fattened, but you see, she failed to push the baby”.
The study explored and presents the childbirth experiences among postnatal mothers and the meaning attributed to such experiences. The themes that emerged majorly focused on childbirth pains and management, institutional care and support, social support, childbirth fears and the meaning attributed to their childbirth experiences.
Childbirth pains and management
The intensity of labour pains, the duration and patterns gave women different birth experiences and responses. The varied experiences were a reflection that each labour and birth a woman goes through is a unique experience even to women who have given birth before [ 27 ].This calls for proper assessment and understanding of the individual intrapartum needs of a woman by the health care providers and emotional support by the birth companion for a positive childbirth experience [ 28 ]. It was noted that people in the communities orient women to consider labour pains natural and normal regardless of their nature and this is intended to build courage and self-confidence of women during birth. Similarly, in a study done in Ghana, a first time mother was told in advance by her mother that labour was painful but should harden and remain strong [ 29 ]. Although women experienced prolonged and exhaustive labour pains with moments of confusion, inability to move, backs being felt in pieces and feelings of despair, divergent feelings of yes and no need regarding biomedical pain relief administration during childbirth were elicited. The women that were not in favour of the administration of drugs for pain relief simply felt birth pains were natural and medicine could not stop them. These expressions were of no surprise given that use of drugs to control pain during childbirth is still a rare occurrence in the country’s health care system like it is reported in other settings [ 29 ]. The evidence that none of the mothers received medication for pain relief despite a few of them expressing desire to have it, was a clear indication of limited access to such interventions. The women posited that without pain a baby could not come out, an indication of a knowledge gap on use of drugs for pain relief during labour. This calls for orientation of women on pain management options to empower them demand for their right of a pain free labourexperience as also recommended by the WHO intrapartum care model of 2018 [ 28 ].
The women’s experiences of care and support varied from positive to negative and non-satisfying. The majority of women had given birth from the Regional Referral Hospital apart from one woman who had given birth from a private maternity centre. The needs and expectations of mothers in labour may seem to be many, however from this study it became apparent that giving attention and listening to women; good interpersonal communication and involving them in their care plans were key; the provision of physical and psychological support and competence in the management of complications were all paramount. The extent to which care met the individual expectations of mothers influenced the individual comments which were either reflective of a positive or negative birth experience. The women who received attention, good care and support expressed comfort and contentment of the hospital services and built high degree of confidence in the service providers and themselves. In a study done in Australia, women who were under supportive midwives felt contented with their childbirth experiences as opposed to those who were not and felt frustrated [ 27 ]. Similar findings have been reported in studies done in Iceland and India, where kindness and supportiveness to women in labour were strongly emphasized and closely related to a satisfying childbirth experience [ 30 , 31 ]. On the contrary, in this study, women who received little attention, minimal technical, physical and psychological support had their birth experiences non-notable. And as such women lost self-confidence, distanced themselves from the care providers and some built bitterness against them. It was also noted that lack of provision of adequate information about labour processes and progression, poor communication and low involvement of mothers in their plans of care deprived them of full situational control and increased anxiety, stress and other emotional tendencies. Such findings are strongly backed by studies [ 27 , 32 ], in which involvement of mothers in decision making during childbirth increased self-confidence, self-esteem, feelings of being in control and felt they had accomplished a task. These aspects of care are far reaching [ 28 ] that a mother, who misses them, will register a gap and a negative childbirth experience. This therefore calls for a positive attitude of a service provider to enhance and promote these indispensable needs during childbirth.
Support from family members (mums, sisters, mothers in-law, aunties, husbands) and friends was strongly noted during this study. Escorting women to the birth places, provision of food and other requirements; rubbing the back, helping the mother to move to and forth were among the physical support given. Psychologically, they were supported through consolation and counseling and orientation on labour pains before or during labour. Social support in this study was strongly noted as a source of comfort, encouragement and hope to the mothers as strongly supported in other studies [ 33 ].
The presence of the male partner in the labour ward and his proximity to the spouse was appreciated by some women while others felt comfortable when their spouses were at a distance for fear of shifting blame to their male partners as trouble causers. Such divergent views and feelings about the men’s availability in labour wards have been cited in [ 34 ] in which some women expressed fear of their partners being impolite and non-loving to them while others were comfortable and in agreement with the practice. In Uganda, the practice of a female partner being with her spouse in a labour suite is just starting (mainly in private hospitals) and thus it is new to most women and men contrary to the developed world where the culture is deeply embedded in their care [ 35 ]. In a Swedish study [ 36 ] men from other countries appreciated the Swedish culture that transformed them from being “men at a distance” and women at “close proxy” to “a family” at the centre of every family member’s health concerns including childbirth. In this study, most participants had given birth from a government hospital and like most other government health facilities in this country, it had a general labour ward whose admission capacity was up to six mothers at a single moment. This minimized the space for a single laboring woman whose privacy was fragile and only protected by a curtain in between the beds. This further explains the low number of male partners and their low levels of involvement in labour processes for their female partners especially in the labour wards. Similar findings of a non-supportive environment for male involvement, have been reported in a study done in Mulago hospital [ 37 ].The findings of the study clearly indicated that mothers in labour currently have two schools of thought regarding the presence of male partners in labour suites. This calls for more research in this area to fully understand the factors that influence male partner involvement in labour and birth processes.
The fears of childbirth reported in this study were majorly associated with the uncertainties of birth outcomes especially women who underwent an operation for they were not sure of the lives of the baby and self; or whether it would result in complications. Similarly, Corbett and Callister [ 30 ] found out that the Tamil Nadu women had fear of “the unknown” as they could not imagine the birth pains, and also feared caesarean birth leading to anxiety. In a Taiwan study [ 38 ] the caesarean births augmented more the risk of stress compared to women who gave birth vaginally and it was thought to be associated with hormonal differences or lack of self-confidence. In a Turkish study, the complications greatly contributed to birth fears [ 39 ]. These fears are further justified by Harrison and Goldenberg [ 40 ] who found out that complications like heamorrhage, embolism, hypovolemic shock, pre-eclampsia and eclampsia contributed to poor or severe maternal outcomes especially in resource limited geographies among caesarean births.
The non-satisfying childbirth experience due to the negative attitudes and practices of the health care providers frightened women and as such they vowed never again to give birth in the public hospitals. Furthermore, the stories the mothers heard from other women about the care and the practices of health care providers in hospital, caused some women to resist moving to hospital with the eventual decision to give birth with the TBA. This puts a woman further at risk and undermines the quality of the outcomes of labour given the limited level of knowledge and skills of the traditional birth attendant [ 41 ].Although labour pains were significantly noted by almost all women, to a lesser extent they were reported to be a source of fear possibly due to the social orientation of women about labour. These findings are contrary to what was found out in a Turkish study where labour pains was the most feared component of childbirth [ 42 ].Generally,fear caused stress and anxieties to mothers, both of which are factors that have been found to distort contractions and prolong labour and render one’s birth experience negative [ 33 ]. Overall, it is important to note, that creating a conducive birthing environment, free of fear, is key in promoting a sense of trust and confidence both in the health care providers and in theservices they offer for a positive childbirth experience.
Meaning attached to childbirth experiences
The meaning of the childbirth experiences captured was two folded. The first one was – the mother’s personal interpretation of her own birth experience and two was how other people in the community interpreted the birth experience she went through. The women drew personal meanings and lessons of their birth experiences mainly from the nature of labour pains they had, the treatment by the service providers, the complications experienced and the labour outcomes. According to their accounts, women felt it was important and safer to deliver in a hospital especially those who had given birth at home and those who got complications like severe bleeding.Such lessons learnt could be helpful to a woman to subsequently make rational decisions regarding the birthing place. On the contrary, in a study done among Hmong women of Vietnam, majority of participants preferred a home birth for fear of loss of control over birth care decisions, limited comfort and loss of the placenta for cultural rituals [ 30 ].Findings also revealed that self-determination, self-confidence, self-belief and perseverance contributed to their successful childbirth. Although these ideologies may sound non- objective, they are important to note for they provide a basis for further assessment of their underlying causes from which objective interventions can be designed to improve childbirth. Self-belief and self-confidence have been found to promote and were closely related to positive childbirth experiences [ 43 ]. The women associated a normal vaginal birth (a birth free of complications) to braveness and being strong as they withstood and tolerated the birth hardships especially contractions. Such beliefs are important to understand by a health care provider so as to provide appropriate counseling to those who may experience complications during childbirth and those who undergo cesarean birth to prevent frustration, loss of self-esteem and feelings of inadequacy.
The cultural and social interpretations of childbirth experiences were the perceived meanings of childbirth by other people. Given the fact that these mothers were living in the same communities, it was speculated that the participants knew or had heard what people say about their birth experiences. According to the accounts of mothers, the majority of meanings were drawn from the type of birth one underwent. Culturally, every woman is expected to be strong, endure with pain and give birth vaginally. So, if a woman gave birth by caesarean, she would be considered bewitched, failed to push (a failure), weak and a woman not good to make a housewife. These findings might be so because in many African cultures, what goes wrong is thought to be an influence of evil spirits. They also believe in big number of children yet a mother, who is operated right from the first child, can safely produce four. Such interpretations may cause loss of self-esteem leading to poor adjustment to motherhood [ 43 ]. Understanding the cultural interpretations of childbirth experiences helps a health care provider to provide emotional support to the sufferers and their families and generally for the decision makers to design interventions that can address knowledge gaps regarding birthing options.
Limitations
Childbirth experiences were got from mothers of parity five and below despite trying hard to look for those ones with parity above five. These possibly would have given different stories regarding childbirth. Literature from Africa on childbirth experiences and their meaning to mothers was limited giving a narrow point of reference when discussing the results in regard to the African context. Therefore, we recommend that subsequent similar or related studies look at settings like Latin America for a broader and closer contextual comparison. The socio cultural interpretations of the childbirth experiences may not fully reflect the views of all the other people in the studied community given the narrow source of the views.
Childbirth experiences were unique and elicited unique feelings, responses and challenges to individual mothers, thus the need for the proper assessment and understanding of women for personalized care. It is important to note that pain management during labour is a necessity and a right of a woman to experience a pain free labour and birth for a positive childbirth outcome for those who embrace it. Creating a good birthing environment with the health care providers that are competent, compassionate and supportive to their clients, builds a sense of trust, and confidence in them and their services and the institution at large which promotes the general wellbeing of a woman at birth. Understanding the societal perceptions of childbirth experiences provides a basis for identifying and designing interventions to support the victimized mothers and the communities to understand childbirth.
Operational definitions
Childbirth experiences: Is an individual woman’s life event that incorporates interrelated subjective psychological and physiological processes, influenced by social, environmental, organizational and policy contexts [ 1 ].
Childbirth : In this study, childbirth referred to labour and birth.
Experiences: the personal lived through encounter of the phenomenon.
Mothers: women who had been pregnant and delivered.
Meaning: were the individual and subjective interpretations of a situation or a happening (her childbirth experiences) by the mother.
Postpartum period: Is the period from one hour following the delivery of the placenta up to six weeks (WHO, 1998). However, in this study the postpartum period referred to the period from one hour after the birth of the placenta up to eight weeks or two months.
Abbreviations
District Health Officer
Focus Group Discussion
Ministry of Health
Semi Structured Interviews
World Health Organization
Young Child Clinic
Larkin P, Begley CM, Devane D. Women's experiences of labour and birth: an evolutionary concept analysis. Midwifery. 2009;25(2):e49–59.
Article Google Scholar
Mensah R, Mogale R, Richter M. Birthing experiences of Ghanaian women in 37th military hospital, Accra, Ghana. International Journal of Africa Nursing Sciences. 2014;1:29–34.
Semenic SE, Callister LC, Feldman P. Giving birth: the voices of orthodox Jewish women living in Canada. J Obstet Gynecol Neonatal Nurs. 2004;33(1):80–7.
Winter C, et al. Depression, pregnancy-related anxiety and parental-antenatal attachment in couples using preimplantation genetic diagnosis. Hum Reprod. 2016;31(6):1288–99.
Article CAS Google Scholar
Wilkinson SE, Callister LC. Giving birth: the voices of Ghanaian women. Health Care Women Int. 2010;31(3):201–20.
Leeners B, et al. Birth experiences in adult women with a history of childhood sexual abuse. J Psychosom Res. 2016;83:27–32.
Nilsson C. The delivery room: is it a safe place? A hermeneutic analysis of women's negative birth experiences. Sex Reprod Healthc. 2014;5(4):199–204.
Waldenström U, et al. A negative birth experience: prevalence and risk factors in a national sample. Birth. 2004;31(1):17–27.
Størksen HT, et al. The impact of previous birth experiences on maternal fear of childbirth. Acta Obstet Gynecol Scand. 2013;92(3):318–24.
Karlström A, Nystedt A, Hildingsson I. The meaning of a very positive birth experience: focus groups discussions with women. BMC pregnancy childbirth. 2015;15(1):251.
Stoll K, Hall W. Vicarious birth experiences and childbirth fear: does it matter how young Canadian women learn about birth? J Perinat Educ. 2013;22(4):226.
Elvander C, Cnattingius S, Kjerulff KH. Birth experience in women with low, intermediate or high levels of fear: findings from the first baby study. Birth. 2013;40(4):289–96.
Muzik M, et al. Mother–infant bonding impairment across the first 6 months postpartum: the primacy of psychopathology in women with childhood abuse and neglect histories. Arch Womens Ment Health. 2013;16(1):29–38.
O’Higgins M, et al. Mother-child bonding at 1 year; associations with symptoms of postnatal depression and bonding in the first few weeks. Arch Womens Ment Health. 2013;16(5):381–9.
Hodnett ED, et al. Continuous support for women during childbirth. Cochrane Database Syst Rev. 2012;10:1–77.
Renfrew MJ, et al. Midwifery and quality care: findings from a new evidence-informed framework for maternal and newborn care. Lancet. 2014;384(9948):1129–45.
Shiferaw S, et al. Why do women prefer home births in Ethiopia? BMC pregnancy childbirth. 2013;13(1):5.
Burns N, Grove SK. The practice of nursing research. Philadelphia: WB. Saunders Company; 1997.
Google Scholar
Callister LC. Making meaning: Women's birth narratives. J Obstet Gynecol Neonatal Nurs. 2004;33(4):508–18.
Smith JA. Qualitative psychology: A practical guide to research methods. London: Sage; 2015.
Tongco MDC. Purposive sampling as a tool for informant selection. Ethnobot Res Appl. 2007;5:147–58.
Morse JM. Data were saturated. Los Angeles: Sage publications Sage CA; 2015.
Browne J, Minichiello V. The social meanings behind male sex work: Implications for sexual interactions. Br J Sociol. 1995;46:598–622.
Elo S, et al. Qualitative content analysis: a focus on trustworthiness. SAGE Open. 2014;4(1):2158244014522633.
Houghton C, et al. Rigour in qualitative case-study research. Nurse researcher. 2013;20(4):12–7.
Yazan B. Three approaches to case study methods in education: yin, Merriam, and stake. Qual Rep. 2015;20(2):134–52.
Murray L, et al. The experiences of African women giving birth in Brisbane. Australia Health Care for Women International. 2010;31(5):458–72.
Oladapo O, et al. WHO model of intrapartum care for a positive childbirth experience: transforming care of women and babies for improved health and wellbeing. BJOG: An International Journal of Obstetrics & Gynaecology; 2018.
Wilkinson S. and Callister L., Perceptions of childbearing among women in the Ashanti region of Ghana . , 2010. 31(3): p. 201–220
Corbett CA, et al. The meaning of giving birth: voices of Hmong women living in Vietnam. Perinat Neonatal Nurs. 2017;31(3):207–15.
Halldorsdottir S, Karlsdottir SI. Journeying through labour and delivery: perceptions of women who have given birth. Midwifery. 1996;12(2):48–61.
Simkin P. Just another day in a woman's life? Women's long-term perceptions of their first birth experience. Part I Birth. 1991;18(4):203–10.
Iliadou M. Supporting women in labour. Health Sci J. 2012;6(3):385.
Singh D, Lample M, Earnest J. The involvement of men in maternal health care: cross-sectional, pilot case studies from Maligita and Kibibi, Uganda. Reprod Health. 2014;11(1):68.
Redshaw M, Henderson J. Fathers’ engagement in pregnancy and childbirth: evidence from a national survey. BMC pregnancy childbirth. 2013;13(1):70.
Ny P, et al. The experience of middle eastern men living in Sweden of maternal and child health care and fatherhood: focus-group discussions and content analysis. Midwifery. 2008;24(3):281–90.
Kaye DK, et al. Male involvement during pregnancy and childbirth: men’s perceptions, practices and experiences during the care for women who developed childbirth complications in Mulago hospital, Uganda. BMC pregnancy childbirth. 2014;14(1):54.
Chen HH, et al. Understanding the relationship between cesarean birth and stress, anxiety, and depression after childbirth: a nationwide cohort study. Birth. 2017;44(4):369–76.
JamshidiManesh M, et al. The process of women’s decision making for selection of cesarean delivery. Iran J Nurs. 2009;21(56):55–67.
Harrison MS, Goldenberg RL. Cesarean section in sub-Saharan Africa. Maternal health, neonatology and perinatology. 2016; 2 (1):6.
Turinawe EB, et al. Traditional birth attendants (TBAs) as potential agents in promoting male involvement in maternity preparedness: insights from a rural community in Uganda. Reprod Health. 2016;13(1):24.
منش, ج, et al. روند تصمیم گیری زنان در انتخاب زایمان به روش سزارین. نشریه پر. ستاری ایران. 2009;21(56):55–67.
Fenwick J, et al. Study protocol for reducing childbirth fear: a midwife-led psycho-education intervention. BMC Pregnancy childbirth. 2013;13(1):190.
Download references
Acknowledgments
The authors would like to thank the Centre of Excellence for Maternal, Newborn and Child Health Research, Makerere University, School of Public Health for the funds that supported the research. Thanks are also due to the administration and staff of Mbale Regional Referral Hospital for their cooperation and support during data collection and the dear mothers for accepting to participate in the study.
Consent for publications
Not applicable.
The Centre of Excellence for Maternal, Newborn and Child Health supported the study from data collection, analysis, interpretation of data and writing the report. The grant further covered the dissemination / sharing of results at the study site and in scientific conferences within the country.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on request.
Author information
Authors and affiliations.
Department of Nursing, Makerere University, College of Health Sciences, P.O Box 7072, Kampala, Uganda
Josephine Namujju, Richard Muhindo, Joyce Nankumbi & Patience Muwanguzi
Department of Clinical Nursing, Muhimbili University of Health and Allied Sciences, Nursing and Midwifery Services Muhimbili Academic Medical Centre, P.O. Box 65427, Dar es Salaam, Tanzania
Lilian T. Mselle
Department of Health, Policy, Planning and Management, Makerere University, College of Health Sciences, School of Public Health, Kampala, Uganda
Peter Waiswa
Global Health Division Karolinska Institutet, Sweden and Leader Makerere University Maternal and Newborn Centre of Excellence and the INDEPTH Network Maternal and Newborn Health Research, Stockholm, Sweden
You can also search for this author in PubMed Google Scholar
Contributions
JN conceived the research idea and participated in the design, coordination of data collection, and drafting of the manuscript. RM participated in refining the research idea and drafting of the manuscript. LTM performed the analysis and participated in refining the presentation of results and their discussion. PW, JN did critical revision of the research work and provided additional inputs and comments for further improvement of the manuscript. PM participated in the refining the research idea and design. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Josephine Namujju .
Ethics declarations
Ethics approval and consent to participate.
Ethical approval was obtained from the School of Health Sciences Institutional Review Board (SHSIRB) of Makerere University College of Health Sciences. Permission to conduct the study was obtained from Mbale Regional Referral Hospital. Postnatal mothers were briefed about the objectives and procedures of the study, the voluntary nature of participation in the study and that they had the right to withdraw at any time. Special permission was obtained from participants to use the audio recorder during interviews and discussions. It was made clear that the information provided would be treated with strict confidentiality and would only be used for research purposes. All participants gave written consent.
Competing interests
The authors declare that they have no competing interests in this section.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License ( http://creativecommons.org/licenses/by/4.0/ ), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated.
Reprints and permissions
About this article
Cite this article.
Namujju, J., Muhindo, R., Mselle, L.T. et al. Childbirth experiences and their derived meaning: a qualitative study among postnatal mothers in Mbale regional referral hospital, Uganda. Reprod Health 15 , 183 (2018). https://doi.org/10.1186/s12978-018-0628-y
Download citation
Received : 01 May 2018
Accepted : 15 October 2018
Published : 03 November 2018
DOI : https://doi.org/10.1186/s12978-018-0628-y
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Experiences
- Postnatal mothers
Reproductive Health
ISSN: 1742-4755
- General enquiries: [email protected]
- <i>Dobbs</i>-Era Policy Has Irrevocably Changed Teenage Pregnancy
Dobbs -Era Policy Has Irrevocably Changed Teenage Pregnancy

T he risk of teenage pregnancy continues to rise at alarming rates. Representing 5% of total births in the U.S. in 2022, there were more than 146,000 teen births —the overwhelming majority of which are oftentimes unintended . Part of this is due to the advancement in our bodily development. In May , 2024, the Harvard T.H. Chan School of Public Health released important data that shows the continued trend of earlier puberty in girls . This, coupled with data showing that more than 30% of teens are having sex (most of the time without contraception), sheds light on just how vital reproductive care and sex education is to young people.
Yet, in the post- Roe , Dobbs abortion-limiting era, we see policies and legislation going beyond abortion restrictions, limiting sex education and contraceptive access . We thus need to ask how Dobbs -era policies will deal with the biology and behavior of puberty to reduce unintended teen pregnancy.
For the past several decades in the U.S., there has been a gradual decline in the age of when girls have their first period, medically known as “menarche.” It has been suggested that weight or body fat content changes may play a role in this phenomenon in children, but other factors, including environmental stress , may also have an impact. The average age for the first period is now just less than 12 years, when most girls are in fifth or sixth grade. In up to 15% of girls, the first menstrual cycle will occur at 10 years old when most girls are just in fourth grade. The trend of earlier puberty is even more pronounced in children of color, as menarche now occurs at about 11 years and six months for Black and Hispanic girls.
Although the proportion of teens reporting sexual activity has dropped slightly over the past few years, data from the 2021 CDC Youth Risk Behavior Survey (YRBS) shows that 30% of high school students have had sex, and 20% are sexually active. Only 50% of these sexual encounters involved condom use, and only 37% of sexually active females used hormonal birth control. Earlier studies of junior high students revealed that 5 to 20% of sixth graders and 14 to 42% of eighth graders engaged in sexual intercourse. Not only do unprotected sexual practices place children at risk for pregnancy, there is also increased risk of sexually transmitted diseases like HIV, Hepatitis C, syphilis, and gonorrhea, which are on the rise in young people.
Read More: What Nebraska’s Sentencing of a Teen Who Used Abortion Pills Might Mean in Post-Roe America
It is estimated that 61% of pregnant teens give birth, 25% have an abortion, and 15% of pregnancies end in miscarriage or stillbirth. Looking at legal abortions in the U.S. in 2021 , individuals less than 15 years of age accounted for 0.2% of pregnancy terminations, and those between 15 and 18 years accounted for 9%. That year, there were about 1,400 abortions in children younger than 15 years and about 56,000 in those between 15 and 18 years, out of the nearly 650,000 performed in the U.S. In coming years, there will likely be fewer teen abortions and more unplanned births, especially for those who cannot travel to other states from the states with abortion bans. And with puberty coming earlier, this issue is expected to have an increasing impact on younger adolescents.
Showing the value of improved contraceptive availability to teens, teen birth rates have remarkably dropped nearly three-fold over the past two decades. The teen birth rate was 61.8 per 100,000 in 1990 and 13.4 per 100,000 in 2022. Yet, among different racial and ethnic groups , teen birth rates are now nearly two-fold higher in Black and Hispanic girls than in white girls, being about 20.3 per 100,000 in Black and Hispanic girls and 9.1 per 100,000 in white girls in 2022. This difference reflects, among other things, differential access to contraception .
Teen pregnancy prevention rests on two essential pillars: education and contraceptive availability. Abundant evidence shows that teen contraceptive use —including IUDs, long-acting reversible contraception (LARC), oral contraceptives, and condoms—have an excellent safety and efficacy profile if used correctly. However, teen contraceptive access varies from state to state. In 27 states and the District of Columbia , teens can obtain medical contraceptives without parental or legal guardian consent . In other states, minors may consent to contraceptive services without parental permission but with special conditions. When parental consent is required for teen contraception, there is less sexual healthcare service use .
This past year, though, has seen an important milestone related to contraceptive access. In July 2023, the FDA approved the first over-the-counter oral contraceptive, Opill, available at low cost and without age restriction. Emergency contraception, including Plan B, is also available over the counter without age restrictions. Here, too, we have availability challenges, as some pharmacists have refused emergency contraception and birth control to pregnant teens in light of their beliefs.
The second pillar of teen pregnancy prevention is sex education . Recognizing the ages at which children begin puberty, starting sex education in the third or fourth grades, is recommended. There are also well-developed and effective sex education programs for schools that incorporate pregnancy prevention education. These programs also address sexually transmitted disease prevention.
The problem is that not only do these programs vary state to state, many reproductive health programs also begin after children have entered puberty and are not comprehensive . Reflecting policies that seem to counter efforts to reduce abortions, we see that many of the same states that are restricting abortion access are now restricting sex education programs in schools, in part to avoid discussion about the LGBTQIA+ community. Some of these changes are trumpeted under calls for “parental rights” or “abstinence promotion.” Whereas abstinence promotion may reach some students, in most situations, this is not a practical teen pregnancy prevention strategy. Many parents are also uncomfortable discussing sex with their children and do not have the background to provide education to children at the level that health professionals can offer, nor can they properly discuss different contraceptive options .
Read More: How Arizona’s Abortion Ballot Measure Could Affect the Presidential Race
There are other potential legal consequences of teen pregnancy that we are seeing with the criminalization of teen abortion assistance. Many individuals who live in states with abortion bans are traveling to other states or using telemedicine for abortion services. Yet, two states, Idaho and Tennessee , will now criminally charge adults who assist minors in obtaining abortions. We have seen similar state-sanctioned anti-parent action against those seeking mutually agreeable, gender-affirming care for their children, showing how some states are legally overriding parental rights on issues that are traditionally between the family and physician.
Following the Dobbs decision, we heard that some states limiting abortion were going to provide additional support to pregnant women and families of unintended pregnancies. That said, it is unclear whether additional services have been provided. States with restrictive abortion laws also have seen increases in children entering foster care , but have historically provided less support for women and children , as well. These facts, in combination with the higher Black teenage pregnancy rates, have led to the notion that abortion bans in states with large Black populations will worsen racial inequities in child welfare systems.
No matter where we live, we need to acknowledge our children’s biological changes and create safe spaces where they are able to learn—and thus prevent—unintended pregnancy. It is not possible to legislate these biological facts away by limiting sex education or altering teen contraceptive availability. Instead, we need to recognize the importance of this issue, especially in the post- Roe era, rather than sliding backward.
More Must-Reads from TIME
- Heman Bekele Is TIME’s 2024 Kid of the Year
- The Reintroduction of Kamala Harris
- The 7 States That Will Decide the Election
- Why China Won’t Allow Single Women to Freeze Their Eggs
- Is the U.S. Ready for Psychedelics?
- The Rise of a New Kind of Parenting Guru
- The 50 Best Romance Novels to Read Right Now
- Can Food Really Change Your Hormones?
Contact us at [email protected]
Painfulness and Happiness of Childbirth Essay
- To find inspiration for your paper and overcome writer’s block
- As a source of information (ensure proper referencing)
- As a template for you assignment
Introduction
Works cited.
Becoming a mom is an extraordinary experience, full of excitement and happiness. Nine months of pregnancy for a woman is a lifetime, during which there is a unique communication with the child, and maternal feelings are formed. The process of giving birth to a baby can and should be one of the most significant and bright moments in life for a woman in labor. To do this, every woman needs to prepare for this magnificent event. Although the birth of a child carries some painful sensations, the birth of a baby can still be the happiest moment in a woman’s life.
Undoubtedly, in my case, childbirth has become one of the most painful but happiest events in my life. The birth of a child takes place in three stages, the first of which is the process of opening the cervix. Mencarini et al. state that it begins when contractions become regular and end with the complete opening of the cervix, and this stage is one of the most painful (7). When the cervix was fully opened and the baby was ready to pass through the birth canal, I was inspired and supported by the realization that very soon, I would see my child and receive my reward for my labors. The second stage is associated with the child’s passage through the birth canal; it begins after the complete opening of the cervix and ends with the birth of a child (Downe et al. 12). It also causes quite a lot of discomfort and physical pain. The last stage is the expulsion of the placenta. It usually goes away quickly and painlessly compared to the previous two.
For me, the primary source of joy was the knowledge of an imminent meeting with my baby, the realization that his first birthday would take place very soon. The completion of pleasure comes at every stage of a child’s life: when he begins to look, walk, talk and laugh. The baby’s birth was an unforgettable moment and very happy not only for me but also for many mothers.
It must be said that childbirth is a physiological process, and, as everyone knows, no physiological function in our body is accompanied by pain, except for complications caused by illness, fear, and tension. Accordingly, in the presence of a positive psychological mood for childbirth, the absence of anxiety and stress, a woman rarely experiences significant discomfort during childbirth (Bayat et al. 2). Thus, the main idea that every woman should learn is that a positive attitude to childbirth, knowledge, and mastery of relaxation methods during childbirth is the key to a happy birth.
All women have the same scenario of development. However, each woman has her version of the scenario. Moreover, if a woman gives birth for the first time, all she feels is a new experience. Therefore, they talk about a situation of some uncertainty in childbirth. Women will need courage and willingness to make decisions according to the problem, here and now (Nejad et al. 1082). A woman needs to work hard mentally and show self-control and patience, but patience is an essential maternal quality.
In conclusion, the birth of a child is quite a painful process for every woman. Nevertheless, the happiness that the newly appeared mother will experience from the baby’s birth will be worth the suffering that she experiences during childbirth. Despite all the difficulties and possible pain, it would be wonderful if every woman experienced the happiness of having a baby. The recommendation that I could give to every woman would be to maintain the motivation to accept and live childbirth.
Bayat, Arezoo, Amiri‐Farahani, Leila, Soleimani, Mehdi, Eshraghi, Nooshin, and Haghani, Shima. “ Effect of short-term psychological intervention on anxiety of pregnant women with positive screening results for chromosomal disorders: a randomized controlled trial .” BMC Pregnancy Childbirth, vol. 21, no. 757, 2021, pp. 1-11. Web.
Downe, Soo, Finlayson, Kenneth, Oladapo, Olufemi, Bonet, Mercedes, and lmezoglu, Metin. “What Matters to Women During Childbirth: A Systematic Qualitative Review.” PLoS ONE , vol. 13, no. 4, 2018, Web.
Mencarini, Letizia, Vignoli, Daniele, Zeydanli, Tugba, and Kim, Jungho. “ Life Satisfaction Favors Reproduction. The Universal Positive Effect of Life Satisfaction on Childbearing in Contemporary Low Fertility Countries .” PLoS ONE , vol. 13, no. 12, 2017, pp. 1-19. Web.
Nejad, Farnaz, Nejad, Fahimeh, Golmakani, Nahid, Khajehpoor, Mahin, and Mayvan, Fatemeh. “The Relationship between Happiness and Fear of Childbirth in Nulliparous Women.” Journal of Midwifery and Reproductive Health , vol. 5, no. 4, 2017, pp. 1082-1089. Web.
- My Monster: The Fear of Being Alone
- Happiness: Common and Personal Criteria
- Japan's Childbirth Delivery System
- Physical and Mental Effects of Childbirth
- The Suez Canal's Geostrategic Importance
- Happiness Areas and Goals in Personal Life
- How Optimism Improves Immunity
- Concepts of Optimism and Hope
- Adolescence and Emotion Relations
- The Unique Feeling of “Home”
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2022, December 3). Painfulness and Happiness of Childbirth. https://ivypanda.com/essays/painfulness-and-happiness-of-childbirth/
"Painfulness and Happiness of Childbirth." IvyPanda , 3 Dec. 2022, ivypanda.com/essays/painfulness-and-happiness-of-childbirth/.
IvyPanda . (2022) 'Painfulness and Happiness of Childbirth'. 3 December.
IvyPanda . 2022. "Painfulness and Happiness of Childbirth." December 3, 2022. https://ivypanda.com/essays/painfulness-and-happiness-of-childbirth/.
1. IvyPanda . "Painfulness and Happiness of Childbirth." December 3, 2022. https://ivypanda.com/essays/painfulness-and-happiness-of-childbirth/.
Bibliography
IvyPanda . "Painfulness and Happiness of Childbirth." December 3, 2022. https://ivypanda.com/essays/painfulness-and-happiness-of-childbirth/.
Log in using your username and password
- Search More Search for this keyword Advanced search
- Latest content
- For authors
- Browse by collection
- BMJ Journals
You are here
- Volume 8, Issue 10
- Women’s psychological experiences of physiological childbirth: a meta-synthesis
- Article Text
- Article info
- Citation Tools
- Rapid Responses
- Article metrics
- http://orcid.org/0000-0002-9614-9496 Ibone Olza 1 ,
- Patricia Leahy-Warren 2 ,
- Yael Benyamini 3 ,
- Maria Kazmierczak 4 ,
- Sigfridur Inga Karlsdottir 5 ,
- Andria Spyridou 6 ,
- Esther Crespo-Mirasol 7 ,
- Lea Takács 8 ,
- Priscilla J Hall 9 ,
- Margaret Murphy 2 ,
- Sigridur Sia Jonsdottir 10 ,
- Soo Downe 11 ,
- Marianne J Nieuwenhuijze 12
- 1 Faculty of Medicine , Universidad de Alcala de Henares , Alcala de Henares , Madrid , Spain
- 2 School of Nursing & Midwifery, University College Cork , Cork , Ireland
- 3 Bob Shapell School of Social Work, Tel Aviv University , Tel Aviv , Israel
- 4 Institute of Psychology , Uniwersytet Gdanski , Gdansk , Poland
- 5 School of Health Sciences , University of Akureyri , Akureyri , Iceland
- 6 Department of Psychology , Universitat Konstanz Fachbereich Psychologie , Konstanz , Baden-Württemberg , Germany
- 7 Hospital Clinic , University of Barcelona , Barcelona , Spain
- 8 Department of Psychology, Faculty of Arts , Charles University , Prague , Czech Republic
- 9 Emory University. Nell Hodgson Woodruff School of Nursing , Atlanta , USA
- 10 School of Health Science , University of Akureyri , Akureyri , Iceland
- 11 University of Central Lancashire , preston , Lancashire , UK
- 12 Research Centre for Midwifery Science , Zuyd University , Maastricht , The Netherlands
- Correspondence to Dr Ibone Olza; iboneolza{at}gmail.com
Objective To synthesise qualitative studies on women’s psychological experiences of physiological childbirth.
Design Meta-synthesis.
Methods Studies exploring women’s psychological experiences of physiological birth using qualitative methods were eligible. The research group searched the following databases: MEDLINE, CINAHL, PsycINFO, PsycARTICLES, SocINDEX and Psychology and Behavioural Sciences Collection. We contacted the key authors searched reference lists of the collected articles. Quality assessment was done independently using the Critical Appraisal Skills Programme (CASP) checklist. Studies were synthesised using techniques of meta-ethnography.
Results Eight studies involving 94 women were included. Three third order interpretations were identified: ‘maintaining self-confidence in early labour’, ‘withdrawing within as labour intensifies’ and ‘the uniqueness of the birth experience’. Using the first, second and third order interpretations, a line of argument developed that demonstrated ‘the empowering journey of giving birth’ encompassing the various emotions, thoughts and behaviours that women experience during birth.
Conclusion Giving birth physiologically is an intense and transformative psychological experience that generates a sense of empowerment. The benefits of this process can be maximised through physical, emotional and social support for women, enhancing their belief in their ability to birth and not disturbing physiology unless it is necessary. Healthcare professionals need to take cognisance of the empowering effects of the psychological experience of physiological childbirth. Further research to validate the results from this study is necessary.
PROSPERO registration number CRD42016037072.
- physiological childbirth
- lived experiences
- pyschological
- empowerment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/ .
https://doi.org/10.1136/bmjopen-2017-020347
Statistics from Altmetric.com
Request permissions.
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
Strengths and limitations of this study
Strict inclusion criteria were applied so that only studies where all women had unmedicated births were included.
Some births had occurred more than 10 years before. Parity was not differentiated as a criteria.
All selected studies came from high-income countries.
All births were attended by midwives and a relatively large number of women included in this study had a home birth.
Introduction
Childbirth is a profound psychological experience that has a physical, psychological, social and existential impact both in the short and long term. 1 It leaves lifelong vivid memories for women. 2 The effects of a birth experience can be positive and empowering, or negative and traumatising. 3–5 Regardless of their cultural background, women need to share their birth stories to fully integrate an experience that is both physically and emotionally intense. 6
Neurobiologically, childbirth is directed by hormones produced both by the maternal and the fetal brain. 7 During childbirth and immediately after delivery, both brains are immersed in a very specific neurohormonal scenario, impossible to reproduce artificially. The psychology of childbirth is likely to be mediated by these neuro-hormones, as well as by particular cultural and personal issues. The peaks of endogenous oxytocin during labour, together with the progressive release of endorphins in the maternal brain, are likely to cause the altered state of consciousness most typical of unmedicated labour that midwives and mothers easily recognise or describe as ‘labour land’, but this phenomenon has received little attention from neuropsychology.
Midwives and obstetricians require a deep understanding of the emotional aspects of childbirth in order to meet the emotional and psychosocial needs of labouring women. Factors that facilitate a positive birth experience include having a sense of control during birth, an opportunity for active involvement in care and support and responsive care from others in relation to women’s experience of labour pain. 8–10 There is limited research on women’s lived experience of physiological childbirth, including their emotional response. 11–13 This lack of knowledge concerning the psychological dimension of childbirth can lead to mismanagement of the birthing process. At the extreme, a lack of understanding of the psychology of childbirth can contribute to a traumatising birth, which can be devastating to women even when the immediate outcome is a physically healthy mother and newborn. 14 When women in labour encounter caregivers who do not incorporate emotional needs into their care, they can experience this as disrespect, mistreatment or in some instances, as a form of abuse 15 or obstetric violence. 16 The problem of disrespect towards women in labour is a growing concern globally, as is also the over-application of medicalised care practices for healthy women. 17–19 Rates for these interventions vary greatly between and within countries. For example, using 2010 Euro-Peristat data, Macfarlane et al 17 (2016) reported on a range in spontaneous vaginal birth from 45.3% to 78.5%. 20
The medical model has traditionally divided labour into stages according to mechanical or physical changes such as dilation of the cervix and descent of the head as depicted on the traditional Friedman’s curve or WHO partograph. 21 However, the subjective, emotional experience of labour does not conform to these mechanical descriptions of the body’s changes. It is questionable that women experience specific stages or phases as traditionally described by professionals. 22 Understanding the psychological experience in physiological childbirth can contribute to enhancing a salutogenic approach to health and can contribute to the promotion of healthy, happy family relationships in the longer term.
The aim of this meta-synthesis is to locate and synthesise published qualitative studies that describe the psychological process of women during physiological childbirth, paying attention to the immanent psychological responses that emerge during the process of labour and birth. We hypothesised that there is a common psychological experience of physiological labour. We focus on labouring women’s thoughts and feelings, and the meanings they ascribe to their perceptions of childbirth process and the surrounding environment, as reaction to both childbirth and to the surrounding environment are part of a single psychological process. We refer to the psychological process in terms of the ‘lived experience’ and thus we adopted a Husserlian a phenomenological approach for the analysis of the data in the included studies.
We undertook a meta-synthesis. This is a process of reviewing and consolidating qualitative research, to create a summary of qualitative findings and allow for the development of new interpretations (Thomas and Harden, 2008). Qualitative synthesis of a number of qualitative studies provides robust evidence to inform healthcare practices. Meta-ethnography was deemed the most appropriate qualitative synthesis approach for this analysis in order to transcend the findings of individual study accounts in developing a conceptual model. 23 This synthesis method has the potential to provide a higher level of analysis and generate new conceptual understandings. 24 The research approach used for this meta-synthesis was the seven-step process described by Noblit and Hare, 25 26 which uses meta-ethnographic techniques like reciprocal and refutational techniques as well as line of argument synthesis. We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statements to inform the meta-synthesis. 27 The research protocol was registered and published in the International Prospective Register of Systematic Reviews. 28
Patients and public were not involved in the design, conception or conduct of this study.
Data sources
A systematic search was conducted in March 2016 and updated in October 2017. The following databases were included: EBSCOhost, including the database MEDLINE, CINAHL, PsycINFO, PsycARTICLES, SocINDEX and Psychology and Behavioural Sciences Collection. The search terms are given in online supplementary appendix 1 . (We used EBSCOhost for the complete search and therefore did not use MeSH terms.) Eligible papers were written in English, Spanish and Portuguese. Five groups of two authors independently read the abstracts and selected the articles, and the decision to include an article was achieved by consensus. When there was disagreement, a third author provided assistance and input. We searched reference lists of the included articles to identify additional articles that were relevant to the study question. We sought suggestions from experts in the field and articles from other sources.
Supplementary file 1
Eligibility criteria for selecting studies.
For the purpose of our study, physiological childbirth was defined as an uninterrupted process without major interventions, such as induction, augmentation, instrumental assistance, caesarean section as well as use of epidural anaesthesia or other pain relief medications. The inclusion criteria were (1) original research of (2) women who had physiological childbirth and (3) described their experiences and behaviours during (4) the whole process of childbirth. Studies were excluded, if the experience of childbirth was (1) described by any source other than the woman who experienced the birth (eg, from healthcare professionals), (2) described only a single stage in the birth process or (3) described births with major medical and surgical interventions (or pain management (eg, caesarean section).
Data extraction and synthesis
Data analysis included the following steps. The first order interpretation involved reading and re-reading all studies to become familiar with their content, feeling and tone. The first author (IO) conducted a line-by-line coding of the findings of all included studies. Quotes, interpretations and explanations in the original studies were treated as data. The coding categories included: feelings, behaviours (actions), signs (eg, pain, contractions), relations (midwife, partner, baby and relatives), time perception, cognitions (thoughts and knowledge) and location (home, water, places, transferring). Based on the emerging data, these coding categories were sorted into (1) early labour, (2) intense labour, (3) pushing, (4) baby out (immediately), (5) placenta and (6) evaluation of the whole birth experience.
To achieve the second and third order interpretation, the research team reflected on the first order interpretations to identify the themes and subthemes that describe the emerging constructs grounded in the primary studies. This process included reciprocal (similarity) and refutational (contradictory) analysis which identified differences, divergences and dissonance between the studies and then to synthesise these translations. Following this reflection process, the research team used a line of argument to create a model that best explains the psychological process of physiological childbirth, as described in the included studies.
Quality assessment
To ensure the quality of the findings in the study, all selected papers were screened on the methodological quality using CASP 29 and subsequently, all the included papers were assessed using consolidated criteria for reporting qualitative research (COREQ) 30 to ensure they had reported all the relevant details of their methodological and analytic approach.
Reflexivity
Throughout the research process, the authors identified and explored their own views and opinions as possible influences on the decisions taken. This was done because of the subjective nature of qualitative research to protect the methodological rigour of the study. All the authors of this paper are part of an EU-funded COST Action specifically examining aspects of physiological birth. The research group have chosen to participate in the COST Action IS1405 Building Intrapartum Research Thorugh Health (BIRTH) because of strong interests in the importance of understanding physiological and psychological processes of childbirth, to enhance the capacity of women to labour and give birth normally where this was possible for them, and where it is their choice to do so. All the authors believe that birth is a profound physiological, psychological and socio-cultural experience for most women and babies.
The research team included authors of multidisciplinary backgrounds. The contribution of each author, coming from different paradigms and perspectives on women’s needs in labour, ensured the interpretation of findings was grounded in the data and came from the data. The use of refutational analyses, as recommended by Noblit and Hare 20 21 minimises the risk of overlooking information because it did not fit with the authors’ pre-conceptions. This strengthens the trustworthiness of this research.
Included studies
The search identified 1520 articles in EBSCOhost. There were 376 duplicates, which were removed, leaving 1144 unique articles in the sample. figure 1 demonstrates the selection process, which resulted in eight included studies. All of the selected studies met the quality screening and assessment criteria. Some papers had to be excluded because just one or a few participants did not have a physiological birth as defined for this study. CASP and COREQ assessments are detailed in the online supplementary files .
Supplementary file 2
- Download figure
- Open in new tab
- Download powerpoint
Flow chart.
The eight included studies involved 94 women, 28 primiparous and 22 multiparous women, although four studies did not identify parity in their sample. Of these, two studies had a mix of primiparous and multiparous women (half each) 17 27 and two studies did not address parity for the sample at all. 28 29 Most of the interviews took place within a year after birth, but some studies had longer intervals, and in two studies, women were interviewed up to 10 or 20 years after birth. 11 31 One study did not identify a time interval between the index birth and the interview. 32 Thirty-nine of the women gave birth at home, four in a primary care unit and 51 in hospital. It seems that midwives were the primary carers of these women. Further characteristics of the studies can be found in table 1 .
- View inline
Characteristics of selected studies
Meta-synthesis analysis
Three main themes emerged: maintaining self-confidence in early labour, withdrawing within as labour intensifies and the uniqueness of the birth experience. A number of subthemes were identified within each of the three main themes, which are listed on table 2 .
Themes, subthemes and studies contributing.
Maintaining self-confidence in early labour
This theme presents women’s experiences when they realised that they were in labour. The accounts indicated that women knew when they were in labour and most preferred to wait calmly for progress, maintaining confidence by keeping a familiar routine and environment.
Experiencing the start of labour
Women described their feelings when they realised that they were in early labour. Some felt excited and others described a lovely feeling, comparing it to Christmas 13 (p. 372). A mixture of feelings emanated from the data at this time, including excitement, happiness, calm, sometimes mixed with apprehension and anxiety. 3 11 33
Women found it important to conserve their emotional strength and to maintain a positive attitude. 3 11 Some described being happy with staying in their own home, and felt it was important to keep calm:
I felt confident by staying in my own living room ( 3 , p724).
They acknowledged the close and trustful relationships in their network at that time in their life. 3 13 31
Thought it was reassuring to be together with family in familiar surroundings ( 3 , p724).
Sharing the beginning of labour
When women recognised the beginning of labour, they shared it with other women. Usually they called their mother or sister, before calling the midwife or the hospital. 12 13 Few asked their midwife to be with them at this point.
At 10 o’clock in the morning I called the hospital. Of course, I had talked to my mom first ( 3 , p274).
They indicated that it was important for them to know their midwife, because it gave them confidence and trust 3 12 13 32 33
Keeping life normal
The most common behaviour at the onset of labour appeared to be continuing with the usual routine. There were many descriptions of wanting to remain at home, taking a shower, being aware of others’ needs (like older children or even pets) and waiting happily. Their own home with their relatives and partners around them 3 11 33 was a tranquil place to be while their contractions were becoming more intense and the pain was increasing. 3 11
I was lying all night and with my labour pains and my dog came and lay by my feet…it was an incredible feeling, it was in September, all the apples in the trees…it was all so silent… ( 31 , p352).
Withdrawing within as labour intensifies
As the labour intensified, women withdrew into an inner world where time seemed to be suspended. Women described how this inner space allowed them to concentrate on the labouring process, and this facilitated the feeling that they could manage. The experience of control was complex and nuanced—for some, the sense of being in control was directed at making all of the decisions and for others, it was achieved by feeling safe enough to hand over control (or guardianship) to the midwife, so that they could retreat into their inner world of labouring.
Accepting the intensity of labour
When contractions became stronger and pain intensified, women felt the need to be fully focused on the physical task. 13 At this point women really needed to be with safe companions in a protected place. This was the moment to contact the midwife and/or move to the hospital.
I’ve got to be somewhere where I can actually allow myself to feel what I am going through ( 13 , p373).
The pain experience was framed by accepting pain as a natural part of childbirth, and this was important for women. 3 32 Two key elements in the response to pain were trusting in the body and working with pain. 3 11 Mobility was important in this phase, and women needed to move around 32 or submerge themselves in water. 34 The following quote is an example of how women framed the pain experience to reduce fear.
I don’t think it is explained very well what the pain is for. People just get frightened of the pain. If they could see it as something useful…the pain is there so as you can help them out, it’s not frightening at all (p58).
Women described their desire to be in control, but this was different for the individual women. For some, control meant staying on top of things and deciding what they needed, whereas for others, control was the decision to hand over management to the midwives. 34
Not having any experience of labour, I needed the midwife to tell me what to do. Because she was in control I felt I was too’ ( 34 , p33).
Women expressed their need for a caring approach. 3 11 13 34 The support from midwives helped women to face the vulnerability they experienced during labour.
Knowing the midwives so well makes you feel quite at ease, if you are scared and you haven t got anyone reassuring you, you are just panicking, and it hurts a lot more ( 33 , p239).
You are so incredibly vulnerable and I feel that you have such a need that someone is kind to you and shows you some interest. All your energy goes into giving birth to this child and you simply don’t have energy left to argue with someone or make a fuss about something. You almost have to take whatever your surroundings offer you ( 11 , p52).
All throughout she said to me: you are coping fine, Linda; I felt assured. That was how she was making me feel calm all throughout she said to me: you are coping fine, Linda; I felt assured. That was how she was making me feel calm ( 33 , p239).
A woman giving birth is perhaps much most sensitive or vulnerable that when she is not in labour. If for example the midwife or member of the staff hurt her in some way or says something inappropriate, then it drastically offsets your labour ( 11 , p52)
They also described how important their partner was.
I felt he was my lifeline, he had the best analgesic effect on me and he did not leave me once ( 31 , p. 352).
Sometimes they needed to be alone with their partners yet still able to reach their midwife whenever they needed. 33 34
I felt like we were doing it ourselves, which was nice. We didn’t feel we needed the midwife all the time but she was there if we did ( 34 , p34).
Going to an inner world
Women described how they withdrew within themselves to an inner world, where they focused on the importance of living just in that moment. Words used included ‘ narrowed ’, ‘ zone ’, ‘faraway place’, ‘another planet’ and ‘ private ’. 11–13 31
Nothing else matters and the universe kind of shrinks to this particular, you know this particular job that you have to do which is you know about birthing your baby( 13 , p373).
Like with both my labours, I took myself away. I need not to have people looking at me ( 12 , p49).
Women described perceptions of an altered or suspended sense of time.
My sense of time was completely lost, as if I had forgotten it in a drawer at home. It was a very strange feeling. There are a lot of people around you and yet you are in your own world. Even if we were in the same room we were not in the same world…’( 11 , p52).
Over time as the intensity of the contractions and the pain increased, women described feelings of fear and desperation. 13 Some felt exhausted and deprived of energy. 11 32 The thought that they could not continue any more, expressing fears of death. 11
I was so optimistic in the beginning of the latter birth…I had given birth before and I survived…so that you believe you will survive. However, in both births I had this feeling for some time that I would never survive this ( 11 , p56).
I was requesting for a caesarean, I was requesting for everything! Because I just wanted to get over with it. I just said I was going to die. At one point I felt like I was going to faint and stuff like that. I said: ‘Please Sandra, I want pain relief.’ I was actually begging her, ‘Please, please, please.’ I said, ‘I’m going to die! I won’t be able to do this! ( 33 , p239).
Coming back to push
When starting to push, time was no longer suspended and women became more active. 11 13
When I started to push, it was as if a curtain was drawn. A totally different perception, suddenly I was awake, alert and quite aware of timing’ ( 11 , p55).
… I was at the top of the mountain when I started to push. And then I had to get down again. And that was it! ( 3 , p725).
Uniqueness of the birth experience
With the birth of their baby women described relief, joy at meeting their baby and sense of transformation.
Reaching the glorious zenith
Directly after birth, women described feelings of pride and joy in achieving and experiencing natural childbirth. 11 13 32 33
So I was brave, I was strong!… So I was like, ‘Yes, I have done it! Yes, I can do it!’ I was so happy. I honestly never had this kind of joy since I was born. I don’t know where this joy came from. I don’t know how to describe the endless joy that came in me ( 33 , p239).
What is most prominent in the birth experience as a whole is the sense of victory, the feeling of ecstasy when the baby is born. That feeling is unique, and in the last birth I was without all medication and therefore I could enjoy this feeling much better. Well, I enjoyed it completely ( 11 , p57).
Women described the intensity of their feelings of childbirth as being their greatest, unparalleled achievement.
It is an intense experience, a powerful life experience. It is naturally magnificent that you, just to find that you are capable of giving birth, to a child, that you can do it. To be such a perfect being that you can do it…the feeling you get when you get your new born child into your arms naturally is indescribable. It is a feeling you cannot compare with anything else. It is awe inspiring 11 (p56).
Women also expressed feelings of spiritual closeness and gratitude.
I had this holiness, being close to the universe. I feel such gratitude for the possibility to give birth at home ( 31 , p350).
Some women were also surprised and satisfied how effectively their body had taken them through the labour 13 and they were proud of how they managed their pain. This ability to manage labour pain positively influenced their confidence in becoming a mother. 33
I can’t really explain. I’m very pleased, very pleased, that I did it naturally. I feel so proud, full of myself. I am very proud to have him naturally. I am very proud even now.( 33 , p239).
However, as well as being a unique and powerful experience, some women also expressed a need for a sense of peace, and of routine to ground themselves in the new reality of motherhood. 32
Meeting the baby
Women described the speed with which they assured themselves that their baby looked normal.
I remember particularly that as soon as the baby is born you think incredibly fast and you look incredibly fast whether there are, without all doubts, ten toes and ten fingers and everything that is supposed to be in place is there and many other things. 11 (p56).
Women with other children were impatient for them to meet their new sibling. It was important for them to involve other family members soon after birth to share this important moment with them. 32
As soon as I had the baby I’d had my bath and everything and my mum and everybody arrived…we were all in the garden with the baby ( 32 , p58).
Women described a sense of being ‘cocooned’ within the family soon after the baby was born 33 and this was expressed in the manner in which the new baby was welcomed by hugs, kisses and expressions of love. 31
By three o’clock everybody had left except for just ourselves, the four of us, the whole family. We were just tucked up across my bed and I think in some ways that was the moment that felt that this is absolutely right. There’s nothing more right in the world. I was just all so peaceful. So why would do anything differently kind of feeling to it ( 29 , p58).
The birth of the placenta was only mentioned in one study. 19 For some women, it was anti-climactic after the birth of the baby, while others considered it a part of the recovery process.
Empowered self
After processing their emotions, women described feeling different. They absorbed new knowledge and understanding about themselves and incorporated this into their sense of self. They talked about their birth as an empowering experience. 12
…I felt I could sense right then, when minutes passed by. I felt that I (tearful) was a little bit different ( 11 p56).
Women linked their pride about coping with pain to feeling strong and confident and to a positive start to new motherhood. 33
When you do that as a woman, you know you can do anything … I realised how everything else in life is easy, if you can do that (enduring 70 hours of no sleep, wild contractions, etc.) you can do anything. I am sad that so many women don’t get to understand this ( 12 , p52).
The empowering journey of giving birth
Constructing a line of argument is the next step in a meta-synthesis based on the first, second and third order interpretations. For this study, the line of argument demonstrated ‘the empowering journey of giving birth’, encompassing the various emotions, thoughts and behaviours that women experience during labour.
Women’s psychological journey originated with telling other women from their social network that labour had started, while staying cocooned in a familiar environment. Most women focused on maintaining self-confidence at the start of labour and tended to withdraw into an inner world as labour became more intense. As birth progressed, women experienced an altered state of consciousness including a change in time perception and intense feelings such as fear of dying. Women described various ways of coping with the pain and keeping control, which paradoxically, included releasing control to the midwife where appropriate. With the urge to push, women felt that once again they became alert and more active. Immediately after the baby was born, feelings of joy and pride were predominant. The journey through childbirth meant a growth in personal strength. Some women described themselves as a changed person in the sense that they felt stronger, empowered and ready to meet the demands of the newborn.
Our study offers new insights into women’s psychological experience of physiologic childbirth as a meta-synthesis on this topic has not been previously reported. We created a model of the emerging psychological pattern of this journey that is designated in terms of emotions and behaviours. Women described birth as a challenging but predominantly positive experience that they were able to overcome with their own coping resources and the help of others. For them, this resulted in feelings of strength to face a new episode in their life with their family. Our findings confirm our main hypothesis: there is a common psychological experience of physiological labour. As far as we are aware, this has not previously been reported using women’s accounts as primary data. Our findings suggest that birth is just as much a psychological journey as a physical one.
Although the whole event does not seem to have been described before on the basis of qualitative evidence, elements of our findings are coherent with those from other studies. The preference for familiarity of environment and people at the start of birth, 35 the altered state of consciousness, 36 37 the different time perception, 38–40 the empowerment 6 41 42 and change 37 43 that come with childbirth have previously been described.
In our meta-synthesis, overall women expressed confidence in their capacity to give birth and to trust in themselves and in the process, despite some apprehension as labour began, and some concerns, including fear of death, during the most intensive stages of labour. Positive perceptions of their own coping strategies and confidence in their ability to go through birth were linked to women’s positive experience of birth. 44
Women’s psychological experience of physiological childbirth is strongly influenced by the people present at their birth. Women indicated that close relatives, mostly their partner and mother, as well as care providers were highly relevant for the way women experienced their birthing process. Women described the presence of their partner as the person with whom they most closely shared their experience and relied on for support, confirming that human birth is a social event. 45 This is consistent with other studies that emphasised the decisive contribution partners can make to feelings of trust 46 47 and the woman’s wish for a physiological birth. 48
Women indicated the midwife’s presence as being critically important. At the beginning of the labour, women tended to want to be alone and at a distance from the midwife, but, as labour intensified, they wanted the midwife to be more visible and present while supporting the woman’s control, or taking control if women wanted to hand it over. Control was a key feature in our study. Over the years various researchers identified different internal and external dimensions of control. 49 50 Women’s internal control includes a sense of self-control, such as thoughts, emotions, behaviours and coping with labour pain. External control is described as the woman’s involvement in what is happening during birth, understanding what care providers are doing and having an influence on the decisions. What seems important to women is not so much ‘having control’, but rather the affective component of control, which is the ‘feeling’ of having influence, 10 being able to have a say in what happens and having caregivers who are responsive to expressed wishes. Women’s external control also seemed to arise from feeling that they were informed and could challenge decisions if the need arose. 49
Mixed feelings, both positive and negative, were expressed regarding labour pain, and this is similar to several studies. 51 Women experienced pain as meaningful in relation to their baby. They recognised its intensity but reframed it positively. This was also the case for other feelings that are usually interpreted negatively (being exhausted, feeling overwhelmed and fear of dying) that were referred to in relation to specific moments of the labour and birth, but not in the global psychological evaluation of the experience once it was over. Pain and coping with pain also contributed to gaining strength to cope with the demands of parenthood. Berentson-Shaw et al 44 indicated that stronger self-efficacy during birth explains a lower level of pain. 44 Rijnders et al 52 showed that women who felt unsatisfied about their coping with pain had more negative emotions about their birth. 52
What this meta-synthesis demonstrates is the enormous importance of having maternity care providers, including midwives, at the birth that are compassionate and support women to keep a sense of control that is adjusted to their personal needs and wishes. Care providers can strengthen women’s sense of coherence in offering them emotional support, stimulating trust and confidence and supporting meaningful others to be there during the birthing process. Labouring women need to be able to create a trustful bond with the midwives and obstetricians attending them that offers reassurance and enables them to feel in control. It may be that women are more likely to experience a psychologically positive physiological birth when they feel that a supportive and compassionate companion or healthcare provider (in the case of the included studies, a midwife) is by their side, and is very sensitive and attentive to their cues. This includes effective responses when the woman needs them, and simple encouragement, information or support to reassure them that what is happening to them is normal. Such support may enable women to trust that they are safe to focus inwards, which facilitates the release of hormones and enables the maternal behaviours that are essential to progress a physiological labour and birth. Midwives and other caregivers, including obstetricians, can facilitate this process by demonstrating empathy, compassion and supporting a woman’s belief in her own ability to birth. These are key skills and competencies identified in midwifery-led care, recommended to be implemented worldwide. 53 These affective skills should be included in midwifery, nursing and medical education so that all caregivers have the same expertise in the emotional care of women during birth.
Most women in this synthesis indicated that, for them, birth was an enriching experience that gave them confidence in their own strength to face the challenges of motherhood. These emotions may be quite different when women are confronted with unexpected complications during childbirth, such as an emergency referral to obstetric care, an assisted vaginal birth or an unplanned caesarean section, which tend to be associated with more negative emotions. 54 55 Some women experience grief following a traumatic birth (which could include a birth without interventions, especially where women feel discounted, or actively abused). This grieving may well be the mourning over the loss of the experience which contributes to feelings of empowerment. 56
This study has several limitations. Close to half of the women in the sample had a home birth (39 of the 94 women). Women wishing a home birth seem to have less worries about health issues or fear of childbirth, and a greater desire for personal autonomy. 57 Women planning a midwife-led birth also have lower rates of interventions which is also linked to positive experiences in birth. 58
The studies included in this meta-synthesis were from high-income countries. The experiences of women in places with low-resourced maternity care systems may be different. Our sample was small and we lacked information on women’s parity, preparation for birth, specific details of supporting professionals, partners and significant others, which can be of major influence on women’s experience of childbirth.
Further research is needed in women from different cultural backgrounds. Additionally, it is of great importance to gain insight into the psychological experience of birth in women with complications during pregnancy or childbirth. As childbirth is a neurobiological event directed by neurohormones produced both by the maternal and fetal brain, 7 further research needs to address the interrelationship between neurohormones, psychological experience and physiological labour and birth. 59 60
Positive, physiological labour and birth can be a salutogenic event, from a mental health perspective, as well as in terms of physical well-being. The findings challenge the biomedical ‘stages of labour’ discourse and will help increase awareness of the importance of optimising physiological birth as far as possible to enhance maternal mental health. The benefits of this process can be maximised through physical, emotional and social support for women, enhancing their belief in their ability to birth and not disturbing physiology unless it is necessary.
Conclusions
Giving birth physiologically in the context of supportive, empathic caregivers, is a psychological journey that seems to generate a sense of empowerment in the transition to motherhood. The benefits of this process can be maximised through physical, emotional and social support for women, enhancing their belief in their ability to birth without disturbing physiology unless there is a compelling need. Healthcare professionals need to understand the empowering effects of the psychological experience of physiological childbirth. Further research to validate the results from this study is necessary.
- Marit Torvik H ,
- Selboe ST , et al
- Schmied V ,
- Wilkes L , et al
- McKenzie-McHarg K ,
- Ford E , et al
- Callister LC
- Karlsdottir SI ,
- Sveinsdottir H ,
- Kristjansdottir H , et al
- Nieuwenhuijze M ,
- Thomson G ,
- Santos MJ ,
- Ruiz-Berdún D , et al
- Lukasse M ,
- Schroll AM ,
- Karro H , et al
- 15. ↵ World Health Organization . WHO recommendations: intrapartum care for a positive childbirth experience . WHO 2018 .
- Declercq E ,
- Cabral H , et al
- Macfarlane AJ ,
- Blondel B ,
- Mohangoo AD , et al
- Skinner J ,
- Halldorsdottir S ,
- Karlsdottir SI
- Barnett-Page E ,
- Liberati A ,
- Tetzlaff J , et al
- Leahy-Warren P ,
- Kazmierczak M , et al
- 28. ↵ CASP . Critical Appraisal Skills Programme (CASP). (Qualitative checklist) . http://www.casp-uk.net/casp-tools-checklists ( accessed Oct 2017 ).
- Sainsbury P ,
- France EF ,
- Lang H , et al
- Sjöblom I ,
- Nordström B ,
- Sandall J ,
- Buckland S , et al
- Holloway IM
- Carlsson IM
- Johnson TR ,
- Callister LC ,
- Freeborn DS , et al
- Lindgren H ,
- Erlandsson K
- Berentson‐Shaw J ,
- Rosenberg K ,
- Trevathan W ,
- Lundgren I ,
- Howarth AM ,
- Treharne GJ
- Kringeland T ,
- Daltveit AK ,
- Whitburn LY ,
- Davey MA , et al
- Rijnders M ,
- Schönbeck Y , et al
- Soltani H ,
- Gates S , et al
- Handelzalts JE ,
- Waldman Peyser A ,
- Krissi H , et al
- Henriksen L ,
- Grimsrud E ,
- Schei B , et al
- Andersson E
- van Haaren-Ten Haken T ,
- Hendrix M ,
- Nieuwenhuijze M , et al
- Maassen MS ,
- Hendrix MJ ,
- Van Vugt HC , et al
- Olza-Fernández I ,
- Marín Gabriel MA ,
- Gil-Sanchez A , et al
Contributors All authors conceived and designed the study. MN and PL-W organised and conducted the search. IO, PL-W, YB, MNJ, EC-M, AS, MK, LT, MM and SSJ participated in the selection of the relevant articles. IO and EC-M performed the quality assessment of the studies. IO did the data extraction from the studies and drafted the manuscript. IO, PL-W, YB, MNJ, AS, MK, SSJ, SIK, PJH and SD interpreted the results, critically revised the manuscript for important intellectual content, and contributed to and approved the final version. MNJ, SD and PL-W supervised the project. YB, PJH, SD, MK, PL-W, MNJ and IO made the changes and corrections suggested by the reviewers.
Funding Eu cost action is 1405 birth: Building intrapartum research through health ( http://www.cost.eu/COST_Actions/isch/IS1405 ).
Competing interests None declared.
Patient consent Not required.
Ethics approval Ethical approval was not required for this meta-synthesis.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional unpublished data only available with authors.
Read the full text or download the PDF:
Click through the PLOS taxonomy to find articles in your field.
For more information about PLOS Subject Areas, click here .
Loading metrics
Open Access
Peer-reviewed
Research Article
What matters to women during childbirth: A systematic qualitative review
Contributed equally to this work with: Soo Downe, Kenneth Finlayson
Roles Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing
* E-mail: [email protected]
Affiliation Research in Childbirth and Health (ReaCH) group, University of Central Lancashire, Preston, United Kingdom
Roles Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing
Roles Conceptualization, Funding acquisition, Supervision, Writing – review & editing
¶ ‡ These authors also contributed equally to this work.
Affiliation UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP), Department of Reproductive Health and Research, World Health Organization, Geneva, Switzerland
Roles Conceptualization, Funding acquisition, Resources, Writing – review & editing
- Soo Downe,
- Kenneth Finlayson,
- Olufemi Oladapo,
- Mercedes Bonet,
- A. Metin Gülmezoglu
- Published: April 17, 2018
- https://doi.org/10.1371/journal.pone.0194906
- Reader Comments
17 May 2018: Downe S, Finlayson K, Oladapo OT, Bonet M, Gülmezoglu AM (2018) Correction: What matters to women during childbirth: A systematic qualitative review. PLOS ONE 13(5): e0197791. https://doi.org/10.1371/journal.pone.0197791 View correction
Introduction
Design and provision of good quality maternity care should incorporate what matters to childbearing women. This qualitative systematic review was undertaken to inform WHO intrapartum guidelines.
Using a pre-determined search strategy, we searched Medline, CINAHL, PsycINFO, AMED, EMBASE, LILACS, AJOL, and reference lists of eligible studies published 1996-August 2016 (updated to January 2018), reporting qualitative data on womens’ childbirth beliefs, expectations, and values. Studies including specific interventions or health conditions were excluded. PRISMA guidelines were followed.
Data collection and analysis
Authors’ findings were extracted, logged on a study-specific data form, and synthesised using meta-ethnographic techniques. Confidence in the quality, coherence, relevance and adequacy of data underpinning the resulting themes was assessed using GRADE-CERQual. A line of argument synthesis was developed.
35 studies (19 countries) were included in the primary search, and 2 in the update. Confidence in most results was moderate to high. What mattered to most women was a positive experience that fulfilled or exceeded their prior personal and socio-cultural beliefs and expectations. This included giving birth to a healthy baby in a clinically and psychologically safe environment with practical and emotional support from birth companions, and competent, reassuring, kind clinical staff. Most wanted a physiological labour and birth, while acknowledging that birth can be unpredictable and frightening, and that they may need to ‘go with the flow’. If intervention was needed or wanted, women wanted to retain a sense of personal achievement and control through active decision-making. These values and expectations were mediated through womens’ embodied (physical and psychosocial) experience of pregnancy and birth; local familial and sociocultural norms; and encounters with local maternity services and staff.
Conclusions
Most healthy childbearing women want a positive birth experience. Safety and psychosocial wellbeing are equally valued. Maternity care should be designed to fulfil or exceed womens’ personal and socio-cultural beliefs and expectations.
Citation: Downe S, Finlayson K, Oladapo O, Bonet M, Gülmezoglu AM (2018) What matters to women during childbirth: A systematic qualitative review. PLoS ONE 13(4): e0194906. https://doi.org/10.1371/journal.pone.0194906
Editor: Mohd Noor Norhayati, Universiti Sains Malaysia, MALAYSIA
Received: November 28, 2017; Accepted: February 22, 2018; Published: April 17, 2018
Copyright: © 2018 Downe et al. This is an open access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: All relevant data are within the paper and its Supporting Information files.
Funding: This work was commissioned to the University of Central Lancashire, UK by the UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP), Department of Reproductive Health and Research, World Health Organization, Switzerland as part of the evidence base preparation for the WHO recommendations on intrapartum care. The development of the WHO recommendations on intrapartum care was financially supported by USAID. OTO, MB, and AMG are paid staff of the Department of Reproductive Health and Research, World Health Organization. SD and KF are members of Research in Childbirth and Health (ReaCH) group, University of Central Lancashire, UK. The manuscript represents the views of the named authors only. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests: The authors have declared that no competing interests exist.
Optimum outcomes for pregnant women and their babies depend on acceptable, affordable, accessible, high quality provision of maternity care during pregnancy, childbirth, and the postnatal period [ 1 ]. However, the overuse of interventions in some contexts, and the underuse in others [ 2 ], along with growing evidence of disrespectful and abusive behaviors in some institutional settings [ 3 , 4 ] demonstrates that many maternity services are not meeting these standards. Good quality intrapartum care is vital, both for women and babies who are healthy, and for the minority who experience complications. Basing maternity service design and care provision on what women want and need is essential to maximize uptake of, and continuing access to, service provision [ 5 ]. If local maternity care provision is limited, women may report that they are satisfied, even if they have had poor quality care, as they will not be aware of any better alternatives. Finding out what matters to women about labour and birth (rather than only asking about their actual experiences of intrapartum care) offers the potential to establish what women value, irrespective of what is actually on offer. This could provide a basis for service improvement, locally, and internationally.
Transformational health care, as envisioned by the Global Strategy for Women’s, Children’s and Adolescent Health [ 6 ], requires maternity services to go beyond survival during childbirth. Understanding what outcomes are important to women is critical to developing clinical guidelines and policies that are women-centered, and that are more likely to ensure that women, babies and families thrive as well as survive following childbirth, with the ultimate aim of positive transformation of their lives, and those of their families and communities, in the short and longer term. The objective of this review was, therefore, to explore what matters to healthy women in relation to labour and birth. The findings have informed the framing and development of WHO intrapartum guideline recommendations, and the scope of outcomes to assess optimal intrapartum maternity care in future.
We conducted a systematic qualitative review in accordance with the PRISMA guidelines (See S1 Table for PRISMA Checklist). We included studies where the focus was on healthy pregnant women, who are the majority of those accessing intrapartum care around the world. Study assessment included the use of a validated quality appraisal tool [ 7 ]. Meta-ethnographic techniques [ 8 ] were used for analysis and synthesis, and GRADE-CERQual [ 9 ] was applied to the resulting themes.
Reflexive note
In keeping with quality standards for rigor in qualitative research [ 7 ] the review authors considered their views and opinions on intrapartum care as possible influences on the decisions made in the design and conduct of the study, and, in turn, on how the emerging results of the study influenced those views and opinions. All authors believed at the outset that most maternity care around the world is currently designed to maximize efficiency and to manage risk through precautionary interventions, with less emphasis on the experience of labour and birth for the mother, baby, and attending birth companions. All believed that positive labour experiences are important for the wellbeing of the mother, baby, and the family, in the short and longer term. Refutational analytic techniques [ 8 ] were therefore used to minimize the risk that these pre-suppositions would influence the analysis and the interpretation of the findings.
Search strategy
An example of the search terms used is given in Fig 1 .
- PPT PowerPoint slide
- PNG larger image
- TIFF original image
https://doi.org/10.1371/journal.pone.0194906.g001
In summary, the search terms were run in four broad strings covering population, intervention, outcome, and study type, with a view to capturing a wide selection of relevant studies. The terms were developed following a number of a priori scoping exercises across several databases. Where possible, relevant qualitative research limiters were used (e.g. Clinical Queries—Qualitative: Best Balance) to ensure that searches for qualitative studies were optimized. In instances where preliminary searches generated more than 3000 hits the Boolean operator ‘NOT’ was used to exclude studies that were unlikely to relate to the topic of interest. For example, NOT breastfeeding or breast-feeding or diabet* or contracepti* or HIV or anomol* [Ti,Ab]
Inclusion/Exclusion criteria
No language restrictions were applied. Titles and/or abstracts of potentially relevant studies published in languages other than English were initially translated using a basic translation package (Google Translate). If this process suggested the study would be relevant, the full text was translated in detail by bi or multi-lingual colleagues at The University of Central Lancashire (UCLan) or the World Health Organization (WHO).
Studies published before 1996 were excluded, to ensure that the findings reflect the current generation of women who encounter modern intra-partum care. Only studies where the main focus was the beliefs and expectations of women about labour and childbirth (and not studies where the intent was to collect reflections on intrapartum services actually provided) were included. Studies were included if they reported on women’s views directly (and not through staff or partner opinion, or observational data), and where the views were of the general population of healthy women. Studies were excluded if they focused on a particular intervention (e.g epidural use) or procedure (e.g. episiotomy) or represented the views of specific subgroups of women with particular health problems (e.g. obesity, diabetes, pre-eclampsia, etc;). The views of women who were expecting to have a caesarean section for clinical reasons were also excluded.
KF screened the initial hits against the inclusion criteria and referred any queries to SD for discussion. Abstracts and full text papers were included based on consensus between KF and SD.
Data sources
We searched the following databases: Medline, CINAHL, PsycINFO, AMED, EMBASE, LILACS (for studies conducted in South America) and AJOL (for studies conducted in Africa). Searches were conducted between 25 th July and 4th August 2016. Reference lists of included papers were scrutinized (backchained) and included as appropriate. Zetoc alerts were set up for over 50 relevant journals. Details of included papers were logged on a study specific excel file. An updated search was carried out for papers published between August 2016 and January 2018. The results were used as a confirmability check for the original findings.
Quality assessment
The included studies were subject to quality appraisal using the instrument developed by Walsh and Downe [ 7 ] and modified by Downe et al [ 10 ]. This is a simple appraisal system that rates studies against 11 criteria, and then allocates a score from A-D to each study, based on the extent to which it demonstrated credibility, transferability, dependability, and conformability.
Studies scoring D (‘Significant flaws that are very likely to affect the credibility, transferability, dependability and/or confirmability of the study’) were excluded on quality grounds. [See S1 Appendix for details of Quality Assessment]
Analytic strategy
The analytic process followed the method of Noblitt and Hare [ 8 ], which is derived from the constant comparison method [ 11 ]. In step one, the included papers were examined, and an index paper was selected, chosen to best reflect the focus of the review [ 12 ]. The themes and findings identified by the authors of this paper were entered onto a spreadsheet, to develop an initial thematic framework. The findings of all the remaining papers were then mapped to this framework, which continued to develop as the data from each paper were added [ 13 ]. This process includes looking for what is similar between papers (‘reciprocal analysis’), and for what contradicts (‘disconfirms’) the emerging findings (‘refutational analysis’). For the refutational process, as we added each included paper to the analysis, we consciously looked for data that could disconfirm our emerging themes, or our prior beliefs and views related to the topic of the review. If any disconfirming data were found, the themes were amended, so that they continued to capture all the data from the papers we had already analyzed, as well as taking account of the new insights. This process also ensured that the final analysis had high explanatory power for all the data. [See S1 Appenedix for details of thematic development]
The themes were all agreed by consensus between KF and SD, and subject to appraisal by all members of the review team. All were directly derived from quote material in more than one of the included studies. They were assessed for confidence in the quality, coherence, relevance and adequacy of the data contributing to them using the GRADE-CERQual tool [ 9 ]. This is a recently developed instrument, derived from the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach used in quantitative effectiveness reviews. The GRADE-CERQual assessment results in a final classification of confidence in the theme in four categories: ‘high’, ‘moderate’, ‘low’ or ‘very low’. [See S1 Appendix for details of CERQual assessments]
All the themes were translated (or synthesized) into a ‘line of argument synthesis’ [ 8 ], based on theoretical concepts that explained the data at a conceptual level. The line of argument is more than the sum of the parts of the review. A robust line of argument has high theoretical transferability beyond the particular included studies, and so it is likely to be applicable in a wider range of settings and circumstances. The line of argument formed the basis for a Statement of Findings that was then used to inform the ‘values’ component of the Evidence to Decision frameworks used as the basis of the development of the WHO Intrapartum Care guideline (2018).
Included studies
The primary search strategy generated a total of 5350 hits, including 10 already known to the authors. Twenty-three duplicate studies were removed, leaving 5327 to be screened. 5217 of these studies were excluded by title or abstract, primarily because they were deemed to be unrelated to the topic of interest. The remaining 110 were taken forward for full text review. A further 71 were excluded at this stage. The reasons for exclusion are shown in Fig 2 .
https://doi.org/10.1371/journal.pone.0194906.g002
Of the 39 full text papers, four were excluded after quality appraisal [ 14 – 17 ]. Two were relatively small Brazilian studies with little or no methodological information [ 14 , 15 ], one was a mixed methods review with limited qualitative data [ 16 ] and one had limited methodological information[ 17 ]. Thirty five papers were included in the final analysis. Post-hoc examination of the four papers excluded on quality grounds indicated that inclusion of the data within them would not have changed the final themes, line of argument, or Summary of Findings statement.
There were no additional studies from the Zetoc alerts.
The updated search generated 26 hits (after screening by title) and a further 2 studies were identified [ 18 , 19 ].
Characteristics and quality of included studies (primary search).
The characteristics and quality of the 35 included studies were tabulated, and are summarized in Table 1 .
https://doi.org/10.1371/journal.pone.0194906.t001
The date range of publication for the results of the primary search was 1996–2015. All regions of the world were represented. By continent, the largest number of studies were based in Europe (n = 9) [ 20 – 28 ] , (UK x3, Sweden x2, Finland, Iceland, Norway, Turkey), and Asia (n = 9) [ 29 – 37 ], (China x2, India x2, Nepal x2, Bangladesh, Kazakhstan, Thailand). Six were from South America [ 38 – 43 ], (Brazil x4, Chile, Ecuador), four from North America [ 44 – 47 ], (Canada x2, USA x2), four from Australasia [ 48 – 51 ] and three from Africa [ 52 – 54 ], (Ghana x2, Kenya).
Most data were collected by individual interviews and/or focus or discussion groups. The papers incorporated a range of methodological approaches from relatively small phenomenological studies, to qualitative analysis of free text survey responses. They represented the views of more than 1800 women, from a wide range of ethnic backgrounds, ages (14–49) and socio-demographic groups. The quality was mostly moderate to high (B or above).
The eligible papers from the updated search were scrutinised to assess similarities or differences between the results generated from the primary review, and the themes and findings in the more recent studies.
Table 2 presents the themes emerging from the synthesis of the data, along with codes, subthemes, and related quotes from the included studies, and the GRADE-CERQual rating of the sub-themes (‘evidence statements’). The numbers used in this table are indexed to the appropriate study in superscript in the reference list below.
https://doi.org/10.1371/journal.pone.0194906.t002
The findings suggest that, with high or moderate confidence, most women around the world hope for a labour and birth experience that enables them to use their inherent physical and psychosocial capacities to labor and give birth to a healthy baby in a clinically, culturally, and psychologically safe environment with continuity of practical and emotional support from a birth companion(s), and with kind, sensitive clinical staff, who provide reassurance and technical competency. Most women place a high value on their capacity to give birth physiologically (expressed variously as ‘normal’ or ‘natural’, or without technical or pharmacological interventions) for the short and longer term physical and psychological wellbeing of themselves, their baby and their family; however, they also acknowledge that birth can be an unpredictable and potentially frightening event, and that they may need to ‘go with the flow’. Even where intervention is needed or wanted, women usually wish to retain a sense of personal achievement and control by being involved in decision making.
This is summarized in three overarching themes: Hoping for a positive birth experience : anticipating triumph and delight , fearing pain and abandonment ; the enduring influence of familial and socio- childbirth norms; and Enacting what matters in the context of what is available .
These themes generated the following line of argument:
For most childbearing women across the world, there is inherent value in being able to use one’s own physical and psychosocial capacities to labour, and to give birth to a healthy baby, even when the process is unpredictable and painful. Beliefs about what matters to women are influenced by familial experiences, and local cultural norms and values. The capacity for women to enact what matters to them is affected by anticipated or actual encounters with maternity care staff and services, including the use of desired, required, and/ or feared childbirth interventions.
The themes and findings in the papers included in the updated search confirmed the review findings, suggesting that the analysis is robust, and theoretically transferable to a range of women and settings around the world.
For most of the respondents in the included studies, childbirth was an important experience, which had characteristics of what has been termed ‘liminality’: the transition stage between one state and another during a life-changing rite of passage [ 55 ]. For a small minority, childbirth was simply a physical process that should be conducted as quickly and painlessly as possible. As with other life-transition experiences, many women were fearful in anticipation of the hard work, pain, and uncertainty of labour, but most of them accepted these (potentially extreme) difficulties as part of the necessary process of achieving a positive, or even transformatory, birth experience for themselves and for their baby. Whatever they thought about the nature of birth, women interpreted their expectations of what could and should happen through the lens of family birth stories, and cultural and social norms. Whether women wanted birth over as quickly and painlessly as possible, or whether they understood it as fundamental to their transition to motherhood, they recognized the potential vulnerability of themselves and their baby through the process, and the essential uncertainty about what might happen. This was associated with a strong desire for safe, supportive, kind, respectful and responsive care during labor and birth. These characteristics applied to birth companions, professional and lay care givers, and to the processes and environment of care. The extent to which women could experience what mattered to them was mediated by the nature of the local maternity care provision that was available to them, including the attitudes and behaviours of staff, the quality of the relationship between women and care providers, and the resources and atmosphere of the local facility.
To our knowledge, this is the first meta-synthesis of what matters to women for labour and birth, as opposed to studies of women’s experiences once they have been through the process. Systematic reviews are inevitably dependent on the nature and quality of data that have already been collected and reported. In reviews of qualitative studies, these data have already been interpreted through the lens of what is seen to be important by the primary authors. Too few studies, from too narrow a cultural context, can limit the external transferability of the findings. Although the intent was to only include studies that reported on womens’ a priori views and expectations about what matters to them for labour and birth, independent of any intrapartum care they may have received, in some cases participants views were inevitably informed by their actual experiences.
However, the findings are strengthened by the inclusion of a large number of studies, covering every region of the world, and by the confirmatory analysis carried out as a result of the updated search.
The use of translation software at the inclusion stage of the review could theoretically have led to the exclusion of some relevant papers. In the event, 4 studies (from the primary search) that were included as a consequence of software translation were in languages other than English (3 in Portuguese and 1 in Japanese). The findings of all of these papers were translated by fluent speakers of the relevant language, and they were consistent with the papers written in English. The final analysis was consistent for women in all regions of the world. GRADE-CERQual assessments indicated that confidence in most of the findings was moderate or high, reflecting the quantity and quality of the included studies, and the wide range of settings, viewpoints, and study types included.
The findings largely reinforce the prior beliefs of the authors, which could suggest that different reviewers might have come to different conclusions. However, this risk was limited by the conscious search for disconfirming data to test the emerging codes, subthemes, and main themes.
The findings apply directly to healthy women of a range of parity, and in a range of cultural and economic settings, who are receiving routine intrapartum care. The review did not include studies that were only focused on women with specific health conditions, such as HIV or diabetes, or women from particular marginalised groups, such as those seen as ethnic or cultural outsiders, or very young or very poor women. However, women from some of these groups were part of the respondent sample in some of the included studies, and individual studies of the views of women who are marginalised suggest that the review findings are highly likely to be transferable [ 56 – 59 ].
Facility birth is generally accepted as a solution to persistently high rates of maternal and neonatal mortality and morbidity. However, since Bowser and Hill published their analysis of disrespect and abuse in institutional birth settings, in 2010 [ 60 ], there has been an increasing recognition that, while providing central facilities for maternity care is necessary for the provision of care to women and/or babies with complications, this strategy is not sufficient to ensure optimal outcomes for all women and babies [ 3 ]. Recent WHO antenatal guidelines incorporate evidence from qualitative systematic reviews, indicating that women value the psychological, cultural and emotional experience of pregnancy as well as the health of themselves and their growing baby [ 61 , 62 ]. These reviews have also revealed that women experience pregnancy, birth, and the postnatal period as a psychological and physical continuum, and not as three distinct and un-related states. The current review adds to this body of evidence, by linking what women perceive as a positive labour and birth to local familial and cultural norms that shape the way that childbirth is framed, and by expressing the limitations on how far women believe they can actually enact a positive experience of labour and birth, depending on the available maternity care provision locally.
The findings support the multiple domains of the Lancet Quality of Maternal and Newborn Care Framework [ 5 ], and of the 2015 WHO Quality of Care Framework for Maternal and Newborn Health [ 1 ]. The former takes a human rights perspective, and incorporates a systematic review of what women want and need. The framework recognizes the importance of safe, accessible, evidence based, respectful care provision, and is based on a philosophy of care that optimizes physiological, psychological and cultural norms and values. The latter links the experience of care with provision of care, evidence based practices for routine care and management of complications, actionable information systems and functional referral systems, as well as competent and motivated human resources and essential physical resources.
The findings of this review also complement the Cochrane effectiveness reviews on midwife-led continuity of care [ 63 ] and continuous support in labour [ 64 ]. The finding that most women would prefer not to have labour interventions unless they are necessary for the safety of their baby and/or themselves is reinforced by the recent Lancet Maternal Health series, in which the excessive over-use of intrapartum interventions in both HIC and LMIC countries is shown to be potentially as serious a problem at the population level as the lack of availability of such interventions when they are life-saving [ 2 ].
This review demonstrates that what matters to women in relation to childbirth is underpinned by three phenomena; the physical and psychosocial narture of birth as an embodied experience; local familial and socio-cultural norms that legitimate or reframe expectations about labour and birth; and how maternity care provision enables or restricts what matters. Whether women perceive childbirth to be a transformatory process that has meaning for them and their baby in the short and longer term, or whether they see it as a necessary process that should be completed as quickly and painlessly as possible, maternity services need to be responsive to their values, beliefs, and needs. What matters to women is also what is likely to generate the safest and most humanized maternity care provision, for mother, baby, and the family. There is now sufficient evidence from a wide range of sources to suggest that it is imperative that maternity services recognize the benefits of providing what matters to women (and the risks of not doing so). Crucially, these factors should become a central component of care provision as a matter of urgency to ensure the optimum uptake of effective and respectful maternity care, and, as a consequence, the health of childbearing women and their babies and families, in both the short and longer-term.
Supporting information
S1 appendix. quality assessment, data extraction and cerqual grading..
https://doi.org/10.1371/journal.pone.0194906.s001
S1 Table. PRISMA checklist.
https://doi.org/10.1371/journal.pone.0194906.s002
Acknowledgments
We thank Prof Erika Ota at St Lukes International University in Tokyo for translating the paper published in Japanese[ 35 ]. Mercedes Bonnet at the World Health Organization translated the papers published in Portuguese. With thanks also to Maeve Regan and Hannah Tizzard at The University of Central Lancashire for their help with the searching and screening process and to Claire Glenton and Simon Lewin at the Norwegian Institute of Public Health for their advice on using the GRADE CERQual tool.
- View Article
- PubMed/NCBI
- Google Scholar
- 6. Global Strategy for Women’s, Children’s and Adolescents’ Health (2016–2030). New York: Every Woman Every Child; 2015. Available from http://globalstrategy.everywomaneverychild.org/ [Accessed 19th February 2018]
- 8. Noblitt GW, Hare RD. Meta-Ethnography: Synthesizing Qualitative Studies. Newbury Park, CA: Sage; 1988.
- 11. Strauss A, Corbin J. Grounded Theory in Practice. Thousand Oaks, CA: Sage; 1997
- 13. Schutz A. Collected papers, vol 1. The Hague: Martinus Nijhoff, 1962
- 55. Van Gennep A. The rites of passage. In: Davis-Floyd R, editor. Birth as an American rite of passage. Chicago, IL: University of Chicago Press; 1966.
- 60. Bowser D, Hill K. Exploring evidence for disrespect and abuse in facility-based childbirth: report of a landscape analysis. Bethesda, Maryland, USA: USAID-TRAction Project, Harvard School of Public Health and University Research Corporation, LLC; 2010.
- 62. World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience. 2016; Geneva, Switzerland: World Health Organization.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- J Perinat Educ
- v.9(4); Fall 2000
Why Natural Childbirth?
A reader asks for help in answering the question “Why natural childbirth?” Understanding the simple story of normal, natural birth, what helps and what sabotages nature's plan for birth, and the appropriate use of interventions are discussed and form the foundation for coming to the conclusion that nature's plan makes sense. Women are inherently capable of giving birth, have a deep, intuitive instinct about birth, and, when supported and free to find comfort, are able to give birth without interventions and without suffering.
Question: I have taught Lamaze classes for over 10 years. The epidural rate in the hospital in which I teach is over 90%. Over and over again, I am told that women no longer want natural childbirth and the statistics certainly support that opinion. I need help answering the question, “Why natural childbirth?”
Answer: The first step in finding an answer to the question, “Why natural childbirth?” is to understand the simple (not the medical) story of natural, normal birth. Strangely enough, the more we know about birth, the easier it is to lose sight of how well designed and simple birth actually is. In Lamaze class, our teaching too often focuses on the mechanics of anatomy and physiology and ways to deal with pain rather than telling and retelling the simple story of birth the way it is meant to be.
What Happens in Normal Birth?
In the last month of pregnancy, the cervix softens and ripens like a piece of fruit. Contractions of the uterus become noticeable, and the baby settles into the pelvis. The contractions become stronger, the cervix stretches and opens, and the baby moves lower and rotates, eventually moving down the birth canal. With each contraction, pain sends a signal to the brain and oxytocin is released. With the release of oxytocin, the contractions increase in intensity. As the pain of contractions increases, more oxytocin is released and the contractions become harder.
The pain of labor is what most women worry about. It is important to understand that the pain of the contractions in labor is valuable. It is an important way in which nature actually helps women find their own ways of facilitating birth. In a very real sense, the pain of each contraction becomes a guide for the laboring woman. The positions and activities she chooses in response to what she feels actually help labor progress by increasing the strength and efficiency of the contractions and encouraging the baby to settle in and move down the birth canal. When the pain is entirely removed, the feedback system is disrupted and labor is likely to slow down and become less efficient. As labor progresses and pain increases, endorphins (much more potent than morphine) are released in increasing amounts. The result is a decrease in pain perception, quite naturally. Nature's narcotic! The rising level of endorphins also contributes to a shift from a thinking, rational mind-set to a more instinctive one. Endorphins create a dream-like state, which actually helps women manage the tasks of birthing. Inner experiences become more important than the external environment. As labor progresses and the pain of labor increases, women “go into themselves,” become much less aware and, at the same time, much more focused on the work of labor, and are able to tap into an inner wisdom.
A woman surrounded by family, friends, and health care providers who remind her of the power of labor and encourage her quietly and patiently is a woman who is not afraid. Her support team is totally present and comforts her as she does the hard work of labor. She eats and drinks and, even if labor lasts a long time, she has the energy she needs to persevere. She rests between contractions. No one looks at the clock. Everyone trusts the process of birth and believes that she has the strength and the wisdom to give birth.
In a very real sense, the pain of each contraction becomes a guide for the laboring woman.
The woman moves in response to what she feels. Whether she gives birth in a hospital, birthing center, or at home, she is able to use a wide variety of comfort measures; for example, moving freely, listening to music, taking a shower or bath, and having her feet and hands massaged. She is able to create an environment that is just what she needs as she does the hard work of labor and birth. She pushes her baby down the birth canal, responding now to the pressure of contractions and the baby as he rotates through the pelvis and moves down the birth canal. She moves, changes position, and grunts, sometimes holding her breath—all in response to what she is feeling. In this way, she not only protects the muscles of the birth canal and perineum but also protects her baby as he is born. A great surge of adrenaline insures that the mother is alert, even if her labor has been long. She is totally focused on her baby, ready and eager to embrace him. Baby is eager and alert, too. The stimulation of his journey has primed him for the transition to life outside the womb.
With her baby in her arms, the mother is engrossed, excited, at peace, proud, and astounded at the miracle she has produced. No one tells her what to do. They know that she knows what to do—not because she and her baby have read the books or attended Lamaze class, but because their journey has physically and emotionally prepared them both for this moment. The weight of her baby on her belly helps her uterus contract and expel the placenta. Baby stays warm in his mother's arms. Baby knows just what to do to survive in the world he has entered. He is awake and looks around. Within seconds or minutes, he has his hands in his mouth and is smacking his lips. Unpressured, he slowly but methodically crawls to his mother's breast and self-attaches. As he nurses, his mother's uterus contracts, insuring that bleeding will not be excessive. The two greet each other unhurried, confident, and unpressured. Together, over the next hours and days, they will get to know each other and fall in love.
Nature's Plan
For all of its simplicity, nature's plan for birth actually requires a fair amount of flexibility. Each mother and each baby are different. While the anatomy and physiology are standard, how each labor and birth proceeds is fine-tuned through the active involvement of the laboring woman. All through labor, her body tells her what is happening and helps her discover what she needs to do to help. The active involvement of the laboring woman is a critical piece of nature's plan for birth, and it is the least understood. The hard work of labor is not meant to be accomplished alone. Changing position, avoiding exhaustion, and staying adequately nourished require assistance. So across the world, women giving birth are supported, encouraged, and comforted by family, friends, and professional birth attendants. Giving birth as nature intended is not “biting the bullet and letting it happen.”
The “Everyday Miracle” section of the Lamaze video, Celebrate Birth! (2000) , is an excellent resource to use in your classes. It shares several women's experience giving birth naturally. The commentary highlights the simple story of natural birth. Women are confident, working very hard, supported, and encouraged. “I can do that!” is the exclamation I hear every time I show Celebrate Birth!
In your classes, it is important for you to emphasize that natural childbirth is not about suffering. It is about having the freedom to find comfort in many different ways. Choosing to give birth naturally does not mean that interventions will not be needed or that complications will not occur. Nature's plan for birth includes pleas for help when help is needed. Choosing natural childbirth means that women prepare for the birth of their babies confident in their own ability to give birth, being willing to feel contractions, and finding comfort in response to what they are feeling. It means that they will be surrounded by family, friends, and professionals who will encourage them to trust their inner wisdom. It means that wherever they give birth—hospital, birthing center, or home—they will have the freedom they need to respond to their contractions.
The video Born in the USA (2000) powerfully demonstrates the differences between natural birth and births that become complicated with the cascade of interventions. The women attended by midwives give birth confidently, finding comfort in many different ways, supported and encouraged by family, friends, and their midwife. In stark contrast, the women who give birth attended by physicians in a busy hospital find it difficult to find comfort without medication and appear pressured to give birth quickly. The cascade of interventions is dramatically and realistically presented.
Women know how to give birth without machines, epidurals, and fear.
Why natural childbirth? Ultimately, women find the answer to that question themselves. What they need from us as childbirth educators is to know that nature's design works beautifully. Confident women who are supported and encouraged and who enjoy the freedom to tap into their own wisdom find deep satisfaction in giving birth naturally. The process itself prepares mother and baby perfectly in every way to continue on their journey together.
Some women choose to give birth naturally because they love the challenge. Others find great satisfaction in working hard and “getting the job done.” Many women are eager to avoid anything that might harm their babies or themselves. But the most compelling reason to choose natural childbirth is a universal one. Women know how to give birth without machines, epidurals, and fear. Why natural childbirth? The more important question might be “Why not?”
- Injoy Productions. 2000. Celebrate birth! [Video]. (Available from Injoy Videos, 1435 Yarmouth, Suite 102-B, Boulder, CO 80304; also available from Lamaze International Media Center, www.lamaze.org ) [ Google Scholar ]
- Jarmel M, Schneider K., (Producers). 2000. Born in the USA . [Video]. (Available from Fanlight Productions, 4196 Washington Street, Suite 2, Boston, MA 02131) [ Google Scholar ]
My Birth Story: Moms Share Their Birth Experiences
What to expect birth stories, about what to expect, popular articles, tools & registry.
- Share full article
Advertisement
Supported by
Natural Birth and Breastfeeding: The Decisions That Women Face
Readers discuss a column by Michelle Goldberg, part of a series challenging conventional wisdom.

Natural Childbirth Isn’t Actually the Ideal
Health, safety and happiness are crucial for new parents.
To the Editor:
Re “ Mothers Are Told That Natural Childbirth Is Best. It Isn’t ,” by Michelle Goldberg (“Don’t Tell My Friends, But …” series, Aug. 4):
Ms. Goldberg needs to take a breath. Some of us are old enough to remember when women were subject to all kinds of unnecessary, traumatic and counterproductive measures (strapped down to the delivery table, given routine episiotomies and non-medically indicated C-sections) because they had no choice or power in childbirth. The natural birth movement changed the balance of power for women.
Women still need C-sections. They have options for medication or no medication. They can breastfeed for two years or not breastfeed at all. They control their birth experience. That was not always the case, and it took a lot of fearless advocacy to make it happen.
To associate the natural birth movement with anti-vaxxers is a real disservice to the feminist pioneers who worked so hard to put women back in charge of childbirth.
Carol Brady Atlantic Beach, Fla. The writer is a former executive for nonprofits focused on maternal and child health.
Interesting how the pendulum swings. When I had my first child in the 1970s, my doctor tried to make me feel like a terrible mother because I wasn’t feeding my son puréed meat and vegetables at a month old. I was sent home from the hospital with a month’s supply of corporate baby formula. La Leche League publications were the lone source of helpful information on how to successfully breastfeed your baby — I basically ignored their other ideas about motherhood.
At the time, home births were virtually unheard of in the U.S., and in the hospital, while I managed to escape being put to sleep during labor, nothing like “natural childbirth” was available. My mother, 25 years earlier, had wanted to breastfeed but was talked out of it by her nurses and doctors.
We are having trouble retrieving the article content.
Please enable JavaScript in your browser settings.
Thank you for your patience while we verify access. If you are in Reader mode please exit and log into your Times account, or subscribe for all of The Times.
Thank you for your patience while we verify access.
Already a subscriber? Log in .
Want all of The Times? Subscribe .
I have an only child. Our small family saves money, and traveling is much easier.
- I've only ever wanted one child and am happy with my decision.
- Having one child means our life is easier and cheaper.
- With one child, we get to do more activities and experiences as a family.
" Are you having another one?" is the question every mother is asked after they've had their first child .
"No, I'm one and done," was, and continues to be, my answer. After you say it a few times, people usually get the hint.
I know that for many parents, having one child is not a choice; they would love to add to their family but cannot.
But for me, having one child has been perfect, and I don't regret it. My partner is also happy with our family of three and the life we've created together.
I know my limits
I've always thought that if I did have kids, I would just have one. And after having my daughter 7 years ago, the thought was cemented.
While my pregnancy went OK, giving birth is not an experience I want to repeat. Years on, I'm still recovering physically from issues brought upon by having a baby. With one child, I have the time to exercise and the money to invest in physiotherapy to get my body functioning properly so I can run around after my daughter.
I'm also aware of my parenting limitations. I could probably have another child , but I know I would feel overwhelmed, have less patience, and not be the calm and present mother I want to be.
Our life is easier
In many ways, having an only child is easier.
My partner, daughter, and I love traveling , and not only is it cheaper with just one child, but the logistics are also easier to plan. We all fit together nicely on just one row of a plane and in the back of a cab. We can squeeze into a hotel room or small Airbnb, and the three of us fit easily around a table for two in a café.
Participating in activities or weekend adventures, such as going to the theater, a sports game, or the zoo, is more straightforward and cheaper for our small family.
Related stories
We also save money on things like the weekly grocery bill , school fees, and clothes. The extra money we have allows us to travel and do more things together, creating amazing experiences and memories.
Having siblings isn't a guarantee against loneliness
I know there are many arguments for having more children. They will play together, look after each other, and have a bond for life. Having more children also means extra help as you age , and they'll be there to sort out your house when you die.
These things are all true, but there are counterarguments to them, too.
Having siblings doesn't guarantee help with older parents or funeral arrangements. I've heard many examples of the responsibility falling to one child anyway due to different relationship dynamics, adult responsibilities, and families scattered across the globe.
I have a friend who doesn't have children, and her response to questions about aging and death is that they will pay to put arrangements in place. Similarly, we will put in plans to ensure not all of the burden falls on our daughter.
We get to play, too
I don't agree with the argument that you should have another child just so they have a playmate. My daughter is lucky to have cousins, family friends, sports teams, and schoolmates.
And we get the chance to play with her, too: reading, drawing Lego, puzzles, and board games. We also love cooking and gardening together.
We make a big effort to ensure she's surrounded by other kids and families, and that we get involved in lots of activities.
Having one child is more common now
Back when my parents had children, having two or more was seen as the normal thing to do. Nowadays, I feel less societal pressure to have another kid, and it's more common to see families like ours around.
For us, having an only child was a conscious decision and one that has made our lives easier, cheaper, but also incredibly fun and rewarding.
- Main content
COMMENTS
743 Words. 3 Pages. Open Document. Birth of a child can be such a happy time, especially when the little one is very healthy. We all have seen the movies when a new child is born, some of us are lucky to see it first hand. Some of us do get goose bumps, me being one of them. It is just so exciting to see that little life come out of what has ...
Get original essay. The level of labor deformity hazard is just 4% opposite the 96% of sound babies. By the by, anticipating that guardians still need should get as much birth abandons data as they can keeping in mind the end goal to help decrease the dangers of having an infant with a deformity. Before you intend to get pregnant, watching a ...
The second stage is associated with the child's passage through the birth canal; it begins after the complete opening of the cervix and ends with the birth of a child. Physical and Mental Effects of Childbirth. The most often observed skin alteration during pregnancy and after childbirth, impacting 85% to 90% of women is hyperpigmentation.
As a pregnancy trainer who prepares pregnant women for childbirth, the author wrote her personal childbirth story with an autoethnographic narrative method. Her aim is to help motivate pregnant women preparing for childbirth, health-care professionals preparing those pregnant women, and birthing staff. Keywords: autoethnography, childbirth ...
The first stage of labor is contractions and dilating. This is the start of labor that is true to the dilation of the cervix. This stage is further divided into three other phrases that are namely Latent, Transition, and Active. In latent labor one experiences contractions that are mild and are usually apart from five to thirty minutes.
Essays on Childbirth . Essay examples. Essay topics. 26 essay samples found. Sort & filter. 1 Reviewing Different Childbirth Techniques from Several Countries . 5 pages / 2345 words . Abstract For many years, women have endured the hardships and pain of childbirth. Though a woman's body is built for childbirth, there are several medications ...
The clinical management of labour and childbirth is well understood, but not enough attention is given to making women feel safe, comfortable and positive about their experience.As well as providing essential information on clinical requirements for preventing and managing maternal mortality and morbidity, WHO prioritises the psychological and emotional needs of women giving birth.
IELTS Essay: Childbirth. People nowadays tend to have children at older ages. ... First, giving birth to the child is a hazardous act, when undertaken at a later stage in life. The mortality rate among aging parents, for instance, was much lower in the past, when children were born to families as early as possible. This, however, can still be ...
Free essays on childbirth are academic papers that provide an in-depth analysis of various aspects related to the process of giving birth. These essays may explore topics such as the physical and emotional changes a woman experiences during pregnancy, different methods of childbirth, the role of healthcare providers during labor and delivery, and the impact of cultural beliefs and norms on ...
Childbirth is a crucial concern that should be addressed with diligence since it determines the size and nature of the population. During childbirth, some women decide to give birth at home while others deliver in hospital. In their article, which is referred to as Outcomes of Planned Home Births with Certified Professional Midwives, Johnson ...
Changes in childbirth in the United States: 1750-1950. For most of American history, pregnancy, labor and delivery, and post-partum have been dangerous periods for mother and child. However, starting slowly in the late 18 th century and accelerating into the late 19 th century, labor and delivery radically changed.
Personal Narrative Essay: Giving Birth to my First Child. I used to think that giving birth was overrated and believed that the emotional rollercoaster leading up the birth was insincere. In my opinion, giving birth had always seemed frightening, long and most of all painful. Surprisingly, my whole outlook on giving birth and its emotional ...
The physical and emotional changes of pregnancy and, then, labor, birth, and breastfeeding play vital roles in guiding women on the journey of becoming a mother. Standard prenatal care and medicalized labor and birth interfere in powerful ways with nature's plan and, consequently, women's ability to negotiate this journey.
Hospital Birth vs. Non-Hospital Birth Essay examples According to "Human Sexuality: Diversity in Contemporary America," women and couples planning the birth of a child have decisions to make in variety of areas: place of birth, birth attendant(s), medication, preparedness classes, circumcision, breast feeding, etc.
Birth stories are personal narratives grounded in the pivotal life experience of giving birth. Richly descriptive birth narratives from culturally diverse childbearing women document the importance of listening to the voices of women. Benefits of sharing birth stories include the opportunity for integration of a major event into the framework of a mother's life; the opportunity to share a ...
Childbirth is a significant event in a woman's life and a transition to motherhood. Childbirth experiences are the subjective psychological and physiological processes, influenced by the social and environmental factors [].Birth experiences elicit uncertainties of the next destination with feelings of inabilities [].Labour pain has been regarded as a "well kept - secret" whose true ...
Yet, among different racial and ethnic groups, teen birth rates are now nearly two-fold higher in Black and Hispanic girls than in white girls, being about 20.3 per 100,000 in Black and Hispanic ...
Main body. Undoubtedly, in my case, childbirth has become one of the most painful but happiest events in my life. The birth of a child takes place in three stages, the first of which is the process of opening the cervix. Mencarini et al. state that it begins when contractions become regular and end with the complete opening of the cervix, and ...
Introduction. Childbirth is a profound psychological experience that has a physical, psychological, social and existential impact both in the short and long term.1 It leaves lifelong vivid memories for women.2 The effects of a birth experience can be positive and empowering, or negative and traumatising.3-5 Regardless of their cultural background, women need to share their birth stories to ...
This included giving birth to a healthy baby in a clinically and psychologically safe environment with practical and emotional support from birth companions, and competent, reassuring, kind clinical staff. ... The papers incorporated a range of methodological approaches from relatively small phenomenological studies, to qualitative analysis of ...
Child Birth Essay. 1012 Words3 Pages. Child Birth can be a beautiful, yet unimaginable experience any mother and family member can encounter. It is a process of emotional and social involvements that make-up a natural human being. The familiarity of childbirth can play an important role in life for every individual, especially the mothers who ...
Giving birth as nature intended is not "biting the bullet and letting it happen." The "Everyday Miracle" section of the Lamaze video, Celebrate Birth!, is an excellent resource to use in your classes. It shares several women's experience giving birth naturally. The commentary highlights the simple story of natural birth.
My Birth Story: Moms Share Their Birth Experiences. Every birth story is unique — that's why we asked moms from all over the world to share their experiences of how they welcomed their little ones into the world. No two stories in this series are the same, but each one powerfully illustrates the beauty of birth.
Child Birth Experience Essay. 953 Words4 Pages. Child birth is a very critical event in a women's life, and for her family as well. Imagine having to give birth to a child inside a lobby or waiting area. It's a horrible thought, but unfortunately this is a very real scenario that many underprivileged women in this world have to face.
To associate the natural birth movement with anti-vaxxers is a real disservice to the feminist pioneers who worked so hard to put women back in charge of childbirth. Carol Brady Atlantic Beach, Fla.
Essay by Tegan Forder. 2024-08-17T10:23:01Z An curved arrow pointing right. Share. The ... While my pregnancy went OK, giving birth is not an experience I want to repeat. Years on, I'm still ...